Micronutrient deficiencies: hidden hunger and its prevention in humanitarian crises
- Page updated onJune 29, 2026

Hunger and malnutrition are not just a matter of calories. Millions of people live with a poor and limited diet, which, besides causing acute malnutrition or chronic malnutrition, can also result in deficiencies of essential vitamins and minerals. In fact, this is a problem affecting more than half of children under five and more than two-thirds of women of reproductive age.
Micronutrient deficiencies do not always cause visible or easily recognizable symptoms. This is why they are also known as hidden hunger. However, they have significant consequences, such as an increased susceptibility to infections, defects in child physical and neurocognitive development, blindness, and reduced performance at school or work. Fortunately, there are well-known measures and actions that can help reduce the burden of disease linked to micronutrient deficiencies and their consequences.
Table of contents:
The most prevalent micronutrient deficiencies and their consequences
Most common micronutrient deficiencies today
Although very little information is available on the figures for micronutrient deficiencies, it is estimated that those with the highest prevalence are deficiencies of iron, vitamin A, zinc, vitamin B12, folic acid and vitamin D. In fact, it is believed that at least 56% of children under five suffer from iron, zinc or vitamin A deficiency, and that 69% of women of reproductive age (non-pregnant) suffer from iron, zinc or folic acid deficiency (Stevens et al., 2022).
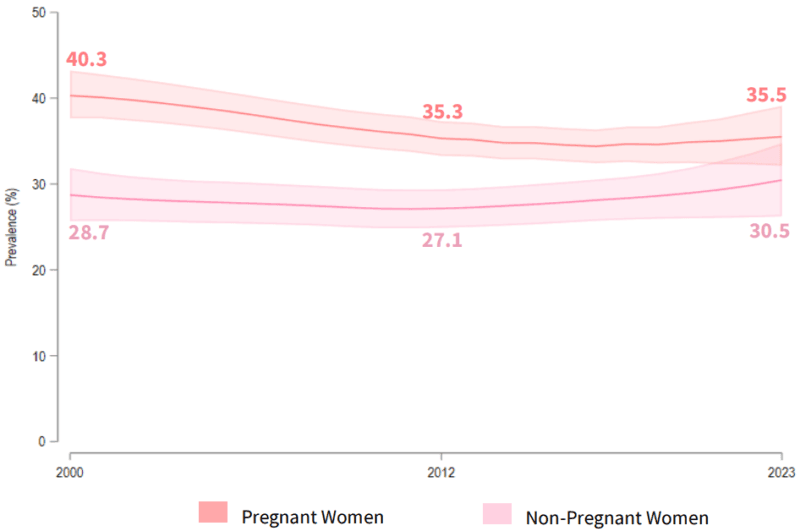
It is also estimated that 35.5% of pregnant women and 30.5% of non-pregnant women suffer from anaemia. This is a figure that appears to be stagnating or even increasing. In any case, it remains far from achieving the SDG target of reducing the prevalence of anaemia in women of reproductive age to 13.8% (WHO, 2025).
These deficiencies constitute a significant public health problem, primarily in sub-Saharan Africa and South-East Asia (Ritchie & Roser, 2017). For example, anaemia affects more than a third of children and pregnant women worldwide. It results from diets poor in iron or vitamin B12, habits that reduce their absorption, and diseases such as malaria. Likewise, vitamin A deficiency weakens the immune system and is the leading global cause of preventable blindness in children. Finally, zinc deficiency has significant effects related to childhood growth stunting and increased risk of illness and infection (Han et al., 2022).
Some micronutrient deficiencies of the past are now exceptional
Although much less common, cases and outbreaks of micronutrient deficiencies that seem a thing of the past in wealthy countries still occur in humanitarian contexts (Jukes, 1989). Examples include scurvy (vitamin C deficiency) (WHO, 1999a), pellagra (vitamin B3 or niacin deficiency), and beriberi (vitamin B1 or thiamine deficiency) (WHO, 1999b).
For example, in 2017 an outbreak of 45 cases of scurvy among young people from South Sudan who were refugees in Kenya occurred (Ververs et al., 2019). Despite receiving partial food assistance and cash transfers to help diversify their diets, they were using this financial support to purchase calorie-dense foods, supplementing the ration they received, which was insufficient. However, they were barely consuming foods rich in vitamin C.
Pellagra occurs only exceptionally, in populations with an almost exclusive diet of maize and in individuals with chronic alcohol consumption (WHO & UNHCR, 2000). However, in the 1990s it was also identified in displaced populations in Malawi, Nepal and Angola. The causes included the reduction of niacin-rich foods in food aid rations, or the distribution of spoiled foods that had lost most of their nutritional value.
There have also been relatively recent cases of beriberi among refugee populations in Thailand, undocumented migrants from Myanmar detained in Malaysia (with a very poor diet in detention), and Rohingya refugees in Indonesia after a long journey by sea.
Preventing micronutrient deficiencies in humanitarian crises
Micronutrient supplementation
The best-documented intervention for addressing micronutrient deficiencies in humanitarian contexts is the use of micronutrient supplements. Although the most common and well-known supplement is iron and folic acid for women and adolescent girls, in humanitarian contexts the use of multiple micronutrient supplements (MMS) is recommended. These include the recommended daily dose of at least 15 vitamins and minerals (Sadler et al., 2024).
There is much debate about the most recommended product for pregnant women. In this group, the benefits of MMS and iron supplements with or without folic acid are similar in terms of anaemia prevention, but MMS have better effects on intrauterine growth. This product, however, was not added to the WHO model list of essential medicines until 2021. Although they are now commonly used in humanitarian contexts, many national guidelines continue to recommend iron and folic acid supplements (Lelijveld et al., 2022). Iron and folic acid supplements are also less expensive than MMS and are often produced within the country itself, which avoids the additional import costs of MMS.
🧠 Let's pause and reflect
Under what circumstances does it make more sense to distribute micronutrient supplements than to invest in improving the diversity and quality of the diet of families affected by a humanitarian crisis?
- 1Think and write your answer.
- 2Click on «Copy and open».
- 3Paste to receive feedback.
📚 This is the NotebookLM for this topic. It uses only carefully selected references. | What is NotebookLM?
Other actions: from fortification to lipid-based supplements and financial assistance
Another recommended approach, in addition to helping improve the diversity of products available to families, is micronutrient fortification. This can be applied to foods such as flours, rice, oils, sugar, salt and condiments. This type of intervention, which should generally be led by national governments, is also applicable to general food distribution programmes for the most vulnerable families in emergencies (UNICEF, 2023).
There are also other alternatives, such as home fortification support or distributions of specialised nutritious foods. One example of these are small-quantity lipid-based nutrient supplements (SQ-LNS), which provide energy, proteins, fatty acids, vitamins and minerals, although they are expensive (UNICEF & GNC, 2024a).
There are other fundamental actions with a very different approach. These involve mainstreaming feminist and gender equality approaches and combining them with cash transfers or actions aimed at women's empowerment (UNICEF & GNC, 2024b). These are interventions that help women gain greater autonomy and economic capacity to supplement their diet with quality products. They also facilitate access to health services, where micronutrient deficiencies can be detected, treated or helped to prevent. In many cases, interventions to promote and protect appropriate feeding, especially in early childhood, also have a positive effect on the prevention of these deficiencies.
References
- Han, X., Ding, S., Lu, J., & Li, Y. (2022). Global, regional, and national burdens of common micronutrient deficiencies from 1990 to 2019: A secondary trend analysis based on the Global Burden of Disease 2019 study. eClinicalMedicine, 44, 101299. https://doi.org/10.1016/j.eclinm.2022.101299
- Jukes, T. H. (1989). The prevention and conquest of scurvy, beri-beri, and pellagra. Preventive Medicine, 18(6), 877–883. https://doi.org/10.1016/0091-7435(89)90023-6
- Lelijveld, N., Brennan, E., Wrottesley, S. V., Akwanyi, B., & James, P. T. (2022). Nutrition of women and adolescent girls in humanitarian contexts: Current state of play. Emergency Nutrition Network. https://www.ennonline.net/humanitariannutritionforwomen
- Ritchie, H., & Roser, M. (2017). Micronutrient deficiency. Our World in Data. https://ourworldindata.org/micronutrient-deficiency
- Sadler, K., James, P., & Mates, E. (2024). Multiple micronutrient supplements in humanitarian emergencies: A state of play report. Emergency Nutrition Network. https://www.ennonline.net/multiple-micronutrient-supplements-in-humanitarian-emergencies
- Stevens, G. A., Beal, T., Mbuya, M. N. N., Luo, H., & Neufeld, L. M. (2022). Micronutrient deficiencies among preschool-aged children and women of reproductive age worldwide: A pooled analysis of individual-level data from population-representative surveys. The Lancet Global Health, 10(11), e1590–e1599. https://doi.org/10.1016/S2214-109X(22)00367-9
- UNICEF. (2023). Large-scale food fortification for the prevention of micronutrient deficiencies in children, women and communities: Guidance note. https://www.unicef.org/documents/large-scale-food-fortification-prevention-micronutrient-deficiencies-children-women-and
- UNICEF & Global Nutrition Cluster. (2024a). Evidence review for the programme guidance to protect the nutrition of women and adolescent girls in humanitarian settings. UNICEF. https://www.unicef.org/media/160221/file/PBWG-Humanitarian-Evidence-review-final.pdf
- UNICEF & Global Nutrition Cluster. (2024b). Programme guidance to protect the nutrition of women and adolescent girls in humanitarian settings. UNICEF. https://www.unicef.org/media/160461/file/Women’s%20nutrition%20humanitarian%20guidance-2024-FINAL-Sept2024.pdf.pdf
- Ververs, M., Muriithi, J. W., Burton, A., Burton, J. W., & Lawi, A. O. (2019). Scurvy outbreak among South Sudanese adolescents and young men — Kakuma refugee camp, Kenya, 2017–2018. Morbidity and Mortality Weekly Report, 68(3), 72–75. https://doi.org/10.15585/mmwr.mm6803a4
- World Health Organization. (1999a). Scurvy and its prevention and control in major emergencies (WHO/NHD/99.11). World Health Organization. https://www.who.int/publications/i/item/WHO-NHD-99.11
- World Health Organization. (1999b). Thiamine deficiency and its prevention and control in major emergencies (WHO/NHD/99.13). World Health Organization. https://apps.who.int/iris/handle/10665/66139
- World Health Organization. (2025). WHO global anaemia estimates: Key findings, 2025. World Health Organization. https://iris.who.int/handle/10665/382291
- World Health Organization & United Nations High Commissioner for Refugees. (2000). Pellagra and its prevention and control in major emergencies (WHO/NHD/00.10). World Health Organization. https://www.who.int/publications/i/item/WHO-NHD-00.10
- World hunger: what it is, causes and why it persists
- What is a famine? Criteria and declaration
- Acute malnutrition (wasting)
- Chronic malnutrition in children (stunting)
- Micronutrient deficiencies: the hidden hunger
- Low birth weight, prematurity and growth retardation
- Breastfeeding and complementary feeding
- Nurturing care for early childhood development
NotebookLM
You can review my literature references on micronutrient deficiencies with this NotebookLM, an artificial intelligence-based research assistant. Do you want to know more?
How to cite this page
Abarca, B. (June 29, 2026). Micronutrient deficiencies: hidden hunger and its prevention in humanitarian crises. Salud Everywhere. https://saludeverywhere.com/en/health-in-humanitarian-crises/micronutrient-deficiencies/