Response to epidemics in humanitarian crises: surveillance, investigation and control
- Page updated onJune 29, 2026

In humanitarian contexts not only does the risk of infections increase, but also the response to epidemics becomes more difficult. It is common for the scarce health personnel to be overwhelmed and the supply of medicines to be cut off. In addition, essential health services such as vaccination, and even essential public health functions are disrupted.
If routine epidemiological surveillance is not guaranteed, an alternative is needed. In such cases, it is recommended to implement an Early Warning Alert and Response System (EWAR) or to strengthen it if one already exists. This will allow signals to be identified, alerts to be managed and outbreak control measures to be guided. The objective is to be able to detect a suspected infectious disease outbreak within 7 days or fewer, notify it within 1 day, and respond within 7 days or fewer with early response actions.
Table of contents:
Frameworks, tools and targets for epidemic outbreak response
Experience with epidemics such as the 2013–2016 Ebola epidemic in West Africa and with the COVID-19 pandemic demonstrated the importance of being prepared. As a result, today there are many reference frameworks and approaches, both for preparedness for public health emergencies and for responding to them once they occur and for evaluating interventions.
Global frameworks for action on public health emergencies
At the 2023 World Health Assembly, the WHO Director-General proposed the creation of an intergovernmental body for strengthening public health emergency prevention, preparedness, response and resilience (HEPR, or Health Emergency Prevention, Preparedness, Response and Resilience) (WHO, 2023a)World Health Organization. (2023, May 5). The World Together: Establishment of an intergovernmental negotiating body to strengthen pandemic prevention, preparedness and response — Progress report by the Director-General (A76/37 Add.1). World Health Organization. https://apps.who.int/gb/ebwha/pdf_files/WHA76/A76_37Add1-en.pdf">(WHO, 2023a)World Health Organization. (2023, May 5). The World Together: Establishment of an intergovernmental negotiating body to strengthen pandemic prevention, preparedness and response — Progress report by the Director-General (A76/37 Add.1). World Health Organization. https://apps.who.int/gb/ebwha/pdf_files/WHA76/A76_37Add1-en.pdf.
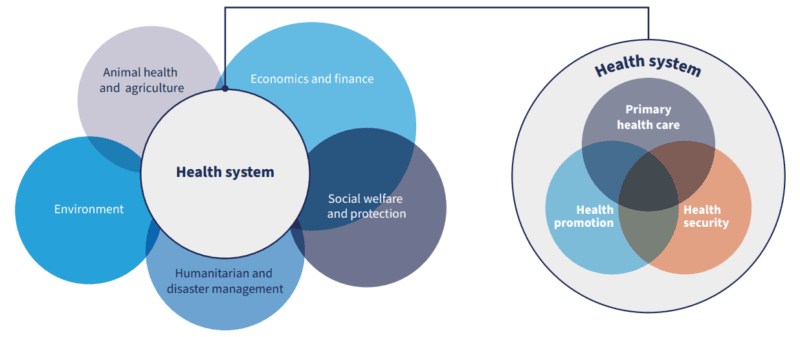
At the heart of the initiative lies the importance of health system capacities (at the intersection of primary care, health promotion and health security) and their interaction with other sectors (WHO, 2023b)World Health Organization. (2023). Strengthening health emergency prevention, preparedness, response and resilience. World Health Organization. https://cdn.who.int/media/docs/default-source/emergency-preparedness/who_hepr_wha2023-21051248b.pdf.
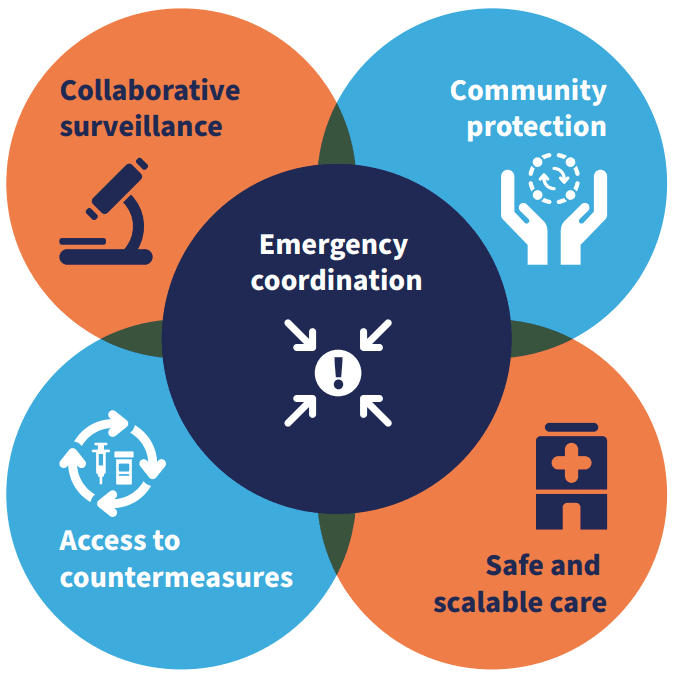
The HEPR framework also establishes the five components ("the five Cs") of public health emergency prevention, preparedness, response and resilience (WHO, 2023b)World Health Organization. (2023). Strengthening health emergency prevention, preparedness, response and resilience. World Health Organization. https://cdn.who.int/media/docs/default-source/emergency-preparedness/who_hepr_wha2023-21051248b.pdf:
- Strong and integrated collaborative surveillance at the national level, with diagnostic and laboratory capacity and joint actions.
- Community protection, with community mobilisation, risk communication, public health interventions and multisectoral socioeconomic protection.
- Safe and scalable health care, with protection of health workers and patients and continuity in the delivery of essential services.
- Access to countermeasures, requiring acceleration of research and development of medicines and vaccines, large-scale production capacity and coordinated supply chains.
- Emergency coordination, with trained and prepared personnel and alert and response systems.
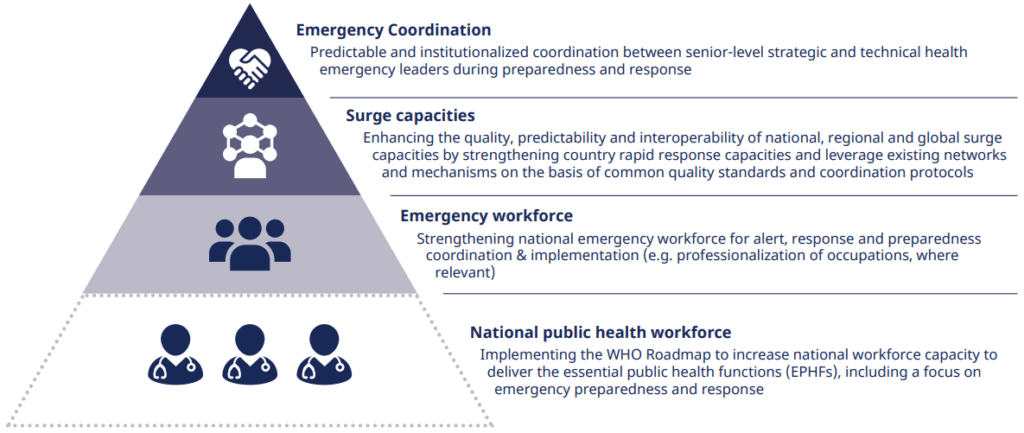
Precisely to enable emergency coordination and collaboration between health personnel and national public health authorities, the HEPR framework also includes the initiative of the Global Health Emergency Corps (GHEC) framework (WHO, 2025a)World Health Organization. (2025). Global health emergency corps framework. World Health Organization. https://www.who.int/publications/b/78043. The premise is that each country should establish a Health Emergency Corps with a well-coordinated, trained and experienced multidisciplinary team, built using a predefined structure common to all countries that allows for their rapid coordination and collaboration under the global GHEC framework.
National frameworks for action on public health emergencies
Other additional frameworks propose how national public health emergency systems and responses should be structured and coordinated, under the umbrella of the HEPR framework and the International Health Regulations.
Among these, the national health emergency alert and response framework (WHO, 2025b)World Health Organization. (2025, October 23). National health emergency alert and response framework. World Health Organization. https://www.who.int/publications/i/item/9789240113893 and the framework proposed by the Global Outbreak Alert and Response Network (GOARN) stand out, covering six technical areas: actor coordination, health information and epidemiology, laboratory and diagnostics, case management, infection prevention and control, and risk communication and community mobilisation (WHO, 2024)World Health Organization. (2024). National outbreak response handbook by the Global Outbreak Alert and Response Network. World Health Organization. https://goarn.who.int/handbook.
When epidemic outbreaks occur in humanitarian crises, these frameworks must be guided by humanitarian principles and adapted to the humanitarian coordination structures already in place in the country (IASC, 2019)Inter-Agency Standing Committee. (2019). Humanitarian system-wide scale-up activation protocol for the control of infectious disease events. https://interagencystandingcommittee.org/iasc-transformative-agenda/iasc-protocol-control-infectious-disease-events-humanitarian-system-wide-scale-activation-2019. Coordination models can vary greatly depending on each context (READY Initiative, 2022a)READY Initiative. (2022, November). Infectious disease outbreak response coordination: An introductory guide for non-governmental organizations. https://www.ready-initiative.org/resource/infectious-disease-outbreak-response-coordination-an-introductory-guide-for-non-governmental-organizations/.
7-1-7: A global target for early detection, notification and response
Despite scientific interest in promoting epidemic response preparedness, it is often difficult to secure its funding, especially in the absence of key progress measures. Faced with this obstacle, and drawing on the successful 90-90-90 target of HIV programmes, a new global objective was proposed in 2021: 7-1-7 (Frieden et al., 2021)Frieden, T., Lee, C., Bochner, A., et al. (2021). 7-1-7: An organising principle, target, and accountability metric to make the world safer from pandemics. The Lancet, 398(10300), 638–640. https://doi.org/10.1016/S0140-6736(21)01250-2:
- A maximum of 7 days to detect a suspected infectious disease outbreak, which requires sufficient material resources, health personnel familiar with case definitions and trained in their detection, and laboratory diagnostic capacity, in order to create an official recorded account of the event.
- 1 day to notify the outbreak to public health authorities..
- A maximum of 7 days to implement effective response measures, including investigation, communication and control measures.
This target not only aligns with other public health emergency response frameworks, but also with different approaches for reviewing performance in outbreak detection, notification and response (Bochner et al., 2023)Bochner, A. F., Makumbi, I., Aderinola, O., Abayneh, A., Jetoh, R., Yemanaberhan, R. L., Danjuma, J. S., Lazaro, F. T., Mahmoud, H. J., Yeabah, T. O., Nakiire, L., Yahaya, A. K., Teixeira, R. A., Lamorde, M., Nabukenya, I., Oladejo, J., Adetifa, I. M. O., Oliveira, W., McClelland, A., & Lee, C. T. (2023). Implementation of the 7-1-7 target for detection, notification, and response to public health threats in five countries: A retrospective, observational study. The Lancet Global Health, 11(5), e703–e712. https://doi.org/10.1016/S2214-109X(23)00133-X.
Reviews of epidemic response actions: before, during and after
Just as important as the quality of epidemic response is the monitoring and analysis of prior preparedness and of the responses themselves, both during and after they take place (WHO, 2025b)World Health Organization. (2025, October 23). National health emergency alert and response framework. World Health Organization. https://www.who.int/publications/i/item/9789240113893. For this purpose, different methodologies exist:
- The International Health Regulations monitoring and evaluation framework allows countries to assess their implementation and capacities.
- Tools and guidelines exist to facilitate conducting an early action review of an epidemic outbreak to assess achievement of the 7-1-7 target (WHO, 2023c)World Health Organization. (2023). Guidance for conducting an early action review (EAR) (WHO/WPE/HSP/CER/2023.1). World Health Organization. https://www.who.int/publications/i/item/WHO-WPE-HSP-CER-2023.1.
- Other methodologies such as intra-action or after-action reviews are more comprehensive evaluations that can be conducted after several months of response or once it has concluded.
Epidemiological surveillance to detect signals and manage alerts
Detection of potential public health events is key to epidemic response
Epidemiological surveillance can be carried out from a functional health information system, or as a component of an EWAR system in emergencies. This system should ideally be integrated into the public health system. It must also be led by national public health authorities, with technical support from the WHO and other actors (WHO, 2023d)World Health Organization. (2023). Early warning alert and response (EWAR) in emergencies: An operational guide. World Health Organization. https://www.who.int/publications/i/item/9789240063587.
In any case, existing epidemiological surveillance should be able to detect signals. Signals are possible public health events, which are not yet verified. They occur when the number of cases of some diseases exceeds alert thresholds. In most cases, it is not possible to monitor all possible diseases. Instead, a set of 8-12 diseases or health conditions considered as priority is selected. To enable signals to be detected, information on these priority diseases will be collected in regular periodic reports. Signals may also be produced when information about potential public health events arrives by any other route. This includes citizen warnings or notifications received through media.
Signal detection is only the first step on the road to a possible response to an epidemic. The second step is alert management. Managing alerts requires verifying signals, analyzing risks, and finally deciding whether to respond to an epidemic.
Once a signal has been detected, its validity must be proactively assessed
The process of signal verification is fundamental in epidemic response. It is what allows false signals to be "filtered out." These can arise from calculation errors, data artefacts, alerts based on false rumours, or repeated alerts, among other causes (WHO, 2023d)World Health Organization. (2023). Early warning alert and response (EWAR) in emergencies: An operational guide. World Health Organization. https://www.who.int/publications/i/item/9789240063587.
For example, a signal may come in the form of a phone call from a nurse at a remote health post. In this hypothetical call, she reports that this morning several users of the post told her that a neighbor's house had a child with a rare paralysis. Hearing that the child could not move his limbs on one side, the nurse thought of a possible case of polio.
Once the signal is detected, verification must be done very quickly, within 24 hours. Generally, a signal can be verified if consultation with the source that reported the signal confirms that the source is reliable. This requires that the clinical case description is reliable and that the epidemiology appears plausible. In other cases, in addition, a signal may be consistent with other signals received in the same period, for example. A verified signal constitutes an event: the manifestation of a disease or a potentially pathogenic event.
It is necessary to determine the risk that each public health event poses to human health
The next step, for each event, is to complete an analysis to determine the risk it poses to human health (WHO, 2023d)World Health Organization. (2023). Early warning alert and response (EWAR) in emergencies: An operational guide. World Health Organization. https://www.who.int/publications/i/item/9789240063587. This is sometimes done locally. In other cases, however, it may require the collection of samples for laboratory analysis. Field visits by specialised rapid response teams may even be necessary. The advantage of having such teams is also that they can quickly initiate an in-depth investigation of the public health event, if needed.
The risk analysis includes:
- A hazard assessment. This analysis addresses aspects such as the number of cases or whether they are laboratory confirmed or not. It also takes into account whether it is a pathology with a high risk of mortality or rapid transmission.
- An exposure assessment. This involves estimating the number of individuals who may have already been exposed to the event. The number that could be exposed in the following days and weeks is also estimated.
- A contextual assessment. This includes aspects such as vaccination coverage, access to water and sanitation or malnutrition rates. It also addresses the availability of health services or the current capacity of the epidemiological surveillance system. This analysis also helps to contextualize the public health event, if it may be affected by conflict or displacement, for example.
The outcome of this risk analysis may determine that the event poses a public health threat. This may be due to its potential impact on human health, its high risk of transmission, or insufficient local capacity to respond. In such cases it is referred to as an alert, indicating that a response is needed.
🧠 Let's pause and reflect
What role can community health workers play in the different components of epidemiological surveillance?
- 1Think and write your answer.
- 2Click on «Copy and open».
- 3Paste to receive feedback.
📚 This is the NotebookLM for this topic. It uses only carefully selected references. | What is NotebookLM?
Responding to epidemics: investigation, communication and control measures
Response to epidemics is the set of public health actions that are implemented following the risk analysis of an alert. The response is not only the implementation of control measures. Before that it may include an in-depth investigation of the epidemic outbreak or the search (active or passive) for cases. It also encompasses monitoring the progress of the outbreak and public communication of the epidemic and its risks.
In-depth research makes it possible to characterize in detail the alert
The in-depth investigation of the epidemic outbreak is sometimes a continuous process starting from the verification of the first signal and risk analysis. Now that there is already an alert, a great deal of work is required to characterize the pathogen and the population at risk. This research will also help to determine the control measures that will be necessary in the response to the epidemic. Therefore, it is important that the investigation be led by an expert in epidemiology.
For the success of an investigation, it is also necessary for the team to include community health workers or community leaders (McGowan et al., 2022)McGowan, C. R., Takahashi, E., Romig, L., Bertram, K., Kadir, A., Cummings, R., & Cardinal, L. J. (2022). Community-based surveillance of infectious diseases: A systematic review of drivers of success. BMJ Global Health, 7(8), e009934. https://doi.org/10.1136/bmjgh-2022-009934. These individuals typically have comprehensive knowledge of the local context and population. It is also essential to have the means to collect samples, send them to designated laboratories and have them analysed there. Laboratory analysis sometimes also includes genomic testing or antibiotic resistance testing. Throughout this process, which can take several days, it may already be necessary to determine some control measures, despite the uncertainty.
A case-finding strategy may be necessary
Outbreak investigation also allows, among other things, for the establishment of an agreed case definition. This will be key for the epidemiological surveillance system to continue with case finding. Case finding strategies depend on the context, the pathogen, or even the evolution of the outbreak (WHO, 2023d)World Health Organization. (2023). Early warning alert and response (EWAR) in emergencies: An operational guide. World Health Organization. https://www.who.int/publications/i/item/9789240063587.
This search can be passive. It is done by asking the community and health personnel to report all suspected cases that come to their attention. At the same time, just in case, they should take protective measures.
An active search can also be employed. This is accomplished with the support of community and community health workers. These volunteers should visit all families believed to have been exposed to the outbreak. They should also follow up on any rumors they hear. In this way they will identify as soon as possible possible cases that would otherwise never be detected in health units.
Monitoring the progress of the epidemic allows to know the attack and case fatality rate
Thanks to the case search, the surveillance system will also be able to produce and periodically update descriptive analyses of the outbreak and its evolution. These analyses make it possible to show how the number of cases evolves along an epidemic curve. They also provide information about the most affected areas or the population groups most at risk, for example.
In addition, monitoring makes it possible to calculate indicators that, during an epidemic, are essential. One of them is the attack rate. It consists of the proportion of new cases in a population over a period. It also helps to calculate the case fatality rate. This is the proportion of cases that die due to a specific condition. All these data can inform key actions to intensify surveillance or concentrate control measures in an area. Moreover, with this information it can be determined whether a response is relevant. If the attack rate is high, it may be necessary to prioritize vaccination, while if the case fatality rate is higher than expected, the quality of medical care may need to be strengthened.
Public communication of information about the epidemic must be done with great care
Responding to an epidemic may require developing a comprehensive strategy for risk communication and community engagement. Messages must include information about the nature of the epidemic, such as the pathogen, risk groups, or affected localities. But that is not all. It is also necessary to communicate the recommended measures to reduce the risk of contagion or in the event of suspected exposure or infection, as well as the available resources (READY Initiative, 2022b)READY Initiative. (2022). Communicating with communities in epidemics and pandemics: Risk communication and community engagement (RCCE) readiness kit. https://www.ready-initiative.org/wp-content/uploads/2022/06/RCCE-Kit_15June-202222-1.pdf.
In any case, messages, by themselves, are never enough. The importance of understanding how communities react to epidemics should never be minimized. It is not easy to deal with some people's fear of contagion, others' low perception of risk or the circulation of rumors and misinformation. Sometimes there is also stigma towards patients, exposed persons or healthcare personnel, or fear of this stigma. It is also important to document and understand possible clashes between recommended control measures and social or religious norms, or mistrust of authorities with little transparency and accountability.
In addition, an adequate risk communication and community mobilization strategy must go hand in hand with a two-way dialogue. This allows the community to participate in the analysis of the situation and the identification of control measures. Moreover, their active participation in the implementation of measures and their monitoring can be a success factor. An example of the risk that exists in epidemics in relation to the way in which the community is connected during the response can be seen in the COVID-19 pandemic. This international public health emergency has had a global impact on the distrust of all types of vaccines and the resurgence of infections.
Responding to epidemics requires control measures adapted to the pathogens and contexts
Possible control measures, depending on the pathogen and the context, include (WHO, 2023e)World Health Organization. (2023). Managing epidemics: Key facts about major deadly diseases (2nd ed.). World Health Organization. https://www.who.int/publications/i/item/9789240083196:
- The reinforcement of health services, both preventive and curative, with a strong emphasis on ensuring accessible primary care.
- Promote the adoption of infection prevention and control measures in healthcare centers. To this end, the availability of personal protective equipment should be ensured. The application of universal precautions should also be promoted and supervised.
- The intersectoral collaboration to ensure water hygiene, animal health or reduction of the risk of further zoonotic transmission, for example.
- Measures aimed at reducing contact and social interactions among the population at risk.
- Isolation measures for persons with confirmed infection (for example in the COVID-19 pandemic).
- The use of vaccines, if available and their use is considered relevant and feasible. They may be important, for example, in epidemics of COVID-19, cholera, measles, Ebola, meningitis, or yellow fever.
- Chemoprophylaxis measures (e.g. in pregnant women at high risk of exposure to malaria).
- Adoption of safe (and dignified) funeral practices, in cases where there is a risk of transmission through contact with the corpse, as in the case of ebola.
All these steps and measures may be impossible without access, preparation and coordination
Each and every one of these measures can pose a tremendous challenge in the midst of a conflict or in displaced populations. They can also do so if the epidemic occurs following an emergency that has deteriorated living conditions, damaged infrastructure and disrupted access to essential services (Marou et al., 2024)Marou, V., Vardavas, C. I., Aslanoglou, K., Nikitara, K., Plyta, Z., Leonardi-Bee, J., Atkins, K., Condell, O., Lamb, F., & Suk, J. E. (2024). The impact of conflict on infectious disease: A systematic literature review. Conflict and Health, 18, 27. https://doi.org/10.1186/s13031-023-00568-z.
There are a thousand other factors that can make managing an epidemiological alert an almost impossible task in a complex humanitarian crisis (Grünewald & Maury, 2020)Grünewald, F., & Maury, H. (2020, April). Epidemics, pandemics, and humanitarian challenges: Lessons from a number of health crises. Groupe URD. https://reliefweb.int/report/world/epidemics-pandemics-and-humanitarian-challenges-lessons-number-health-crises. For example, launching a vaccination campaign against an outbreak may be unfeasible or ineffective when outbreaks are detected late. This is particularly concerning if transmission and contagion is already widespread among populations weakened by forced displacement. An example of this was the case of cholera during the 1994 Goma public health emergency. In addition to the above, building trust towards humanitarian actors among the population can be difficult in highly politicised contexts. Likewise, the entry of medicines, vaccines or medical personnel may be restricted by border closures or access restrictions, among many other possible examples.
Finally, for an adequate epidemic response, adequate health system preparedness before epidemics is also fundamental. Adequate coordination of public health actors during them is equally important. This may require urgently establishing new mechanisms adapted to the crisis, beyond the usual humanitarian coordination mechanisms (Spiegel et al., 2023)Spiegel, P., Esmail, M., Parikh, K., Chatterjee, P., & Quaye, M. (2023, December). Fit for purpose? Global coordination mechanisms of large-scale epidemic response in humanitarian settings -Policy brief-. READY Initiative/Johns Hopkins Center for Humanitarian Health. https://www.ready-initiative.org/wp-content/uploads/2024/01/Ready_Coordination_2_Pager_opt.pdf.
References
- Bochner, A. F., Makumbi, I., Aderinola, O., Abayneh, A., Jetoh, R., Yemanaberhan, R. L., Danjuma, J. S., Lazaro, F. T., Mahmoud, H. J., Yeabah, T. O., Nakiire, L., Yahaya, A. K., Teixeira, R. A., Lamorde, M., Nabukenya, I., Oladejo, J., Adetifa, I. M. O., Oliveira, W., McClelland, A., & Lee, C. T. (2023). Implementation of the 7-1-7 target for detection, notification, and response to public health threats in five countries: A retrospective, observational study. The Lancet Global Health, 11(5), e703–e712. https://doi.org/10.1016/S2214-109X(23)00133-X
- Frieden, T., Lee, C., Bochner, A., et al. (2021). 7-1-7: An organising principle, target, and accountability metric to make the world safer from pandemics. The Lancet, 398(10300), 638–640. https://doi.org/10.1016/S0140-6736(21)01250-2
- Grünewald, F., & Maury, H. (2020, April). Epidemics, pandemics, and humanitarian challenges: Lessons from a number of health crises. Groupe URD. https://reliefweb.int/report/world/epidemics-pandemics-and-humanitarian-challenges-lessons-number-health-crises
- Inter-Agency Standing Committee. (2019). Humanitarian system-wide scale-up activation protocol for the control of infectious disease events. https://interagencystandingcommittee.org/iasc-transformative-agenda/iasc-protocol-control-infectious-disease-events-humanitarian-system-wide-scale-activation-2019
- Marou, V., Vardavas, C. I., Aslanoglou, K., Nikitara, K., Plyta, Z., Leonardi-Bee, J., Atkins, K., Condell, O., Lamb, F., & Suk, J. E. (2024). The impact of conflict on infectious disease: A systematic literature review. Conflict and Health, 18, 27. https://doi.org/10.1186/s13031-023-00568-z
- McGowan, C. R., Takahashi, E., Romig, L., Bertram, K., Kadir, A., Cummings, R., & Cardinal, L. J. (2022). Community-based surveillance of infectious diseases: A systematic review of drivers of success. BMJ Global Health, 7(8), e009934. https://doi.org/10.1136/bmjgh-2022-009934
- READY Initiative. (2022a, November). Infectious disease outbreak response coordination: An introductory guide for non-governmental organizations. https://www.ready-initiative.org/resource/infectious-disease-outbreak-response-coordination-an-introductory-guide-for-non-governmental-organizations/
- READY Initiative. (2022b). Communicating with communities in epidemics and pandemics: Risk communication and community engagement (RCCE) readiness kit. https://www.ready-initiative.org/wp-content/uploads/2022/06/RCCE-Kit_15June-202222-1.pdf
- Spiegel, P., Esmail, M., Parikh, K., Chatterjee, P., & Quaye, M. (2023, December). Fit for purpose? Global coordination mechanisms of large-scale epidemic response in humanitarian settings [Policy brief]. READY Initiative/Johns Hopkins Center for Humanitarian Health. https://www.ready-initiative.org/wp-content/uploads/2024/01/Ready_Coordination_2_Pager_opt.pdf
- World Health Organization. (2023a, May 5). The World Together: Establishment of an intergovernmental negotiating body to strengthen pandemic prevention, preparedness and response — Progress report by the Director-General (A76/37 Add.1). World Health Organization. https://apps.who.int/gb/ebwha/pdf_files/WHA76/A76_37Add1-en.pdf
- World Health Organization. (2023b). Strengthening health emergency prevention, preparedness, response and resilience. World Health Organization. https://cdn.who.int/media/docs/default-source/emergency-preparedness/who_hepr_wha2023-21051248b.pdf
- World Health Organization. (2023c). Guidance for conducting an early action review (EAR) (WHO/WPE/HSP/CER/2023.1). World Health Organization. https://www.who.int/publications/i/item/WHO-WPE-HSP-CER-2023.1
- World Health Organization. (2023d). Early warning alert and response (EWAR) in emergencies: An operational guide. World Health Organization. https://www.who.int/publications/i/item/9789240063587
- World Health Organization. (2023). Managing epidemics: Key facts about major deadly diseases (2nd ed.). World Health Organization. https://www.who.int/publications/i/item/9789240083196
- World Health Organization. (2024). National outbreak response handbook by the Global Outbreak Alert and Response Network. World Health Organization. https://goarn.who.int/handbook
- World Health Organization. (2025a). Global health emergency corps framework. World Health Organization. https://www.who.int/publications/b/78043
- World Health Organization. (2025b, October 23). National health emergency alert and response framework. World Health Organization. https://www.who.int/publications/i/item/9789240113893
- The 21st Century and the resurgence of infections
- International public health emergencies
- Diarrheal diseases and cholera
- Tuberculosis and pneumonia: respiratory infections
- Malaria: progress and challenges toward elimination
- Vaccination in humanitarian emergencies
- Response to epidemics in humanitarian crises
NotebookLM
You can review my literature references on epidemic response in humanitarian crises with this NotebookLM, an artificial intelligence-based research assistant. Do you want to know more?
How to cite this page
Abarca, B. (June 29, 2026). Response to epidemics in humanitarian crises: surveillance, investigation and control. Salud Everywhere. https://saludeverywhere.com/en/health-in-humanitarian-crises/response-to-epidemics-in-humanitarian-crises/