Vaccination in humanitarian emergencies: coverage, campaigns and access to vaccines
- Page updated onJune 29, 2026

Vaccines are essential tools for the prevention and control of infectious diseases. Vaccines have been available for many feco-oral, respiratory or sexually transmitted diseases for years. In addition, new vaccines have continued to be launched, such as those for malaria, Ebola or COVID-19. Other new vaccines are in the process of research and development.
However, in humanitarian emergencies access to vaccines and the ability to use them effectively is reduced. This is in addition to the increased transmission of infectious diseases that also occurs in these contexts. Both, together, result in a worrisome increase in preventable morbidity and mortality. This problem, combined with the other difficulties in ensuring access to essential services in crisis settings, makes it necessary to adapt strategies and programs of vaccination in humanitarian emergencies.
Table of contents:
Why global progress in vaccine coverage has stagnated
Vaccines have saved more lives than any other medical innovation
The first vaccine against smallpox — a disease that has already been eradicated — developed by Edward Jenner in 1796, was followed by many others. In the first half of the twentieth century, vaccines such as that against yellow fever were developed in 1938, earning Max Theiler a Nobel Prize. Advances continued in the second half of the century, with vaccines against poliomyelitis appearing between 1954 and 1960 and against measles in 1963. Since 1986, we have even had the recombinant vaccine against hepatitis B, developed through genetic engineering. These developments continued into the twenty-first century, with the vaccine against human papillomavirus in 2006, followed by a new (and improved) vaccine against meningitis A in 2010, and the more recent vaccines against Ebola, malaria and COVID-19 (WHO, 2022)World Health Organization. (2022). A brief history of vaccination. https://www.who.int/news-room/spotlight/history-of-vaccination/a-brief-history-of-vaccination.
It is estimated that since 1974 vaccines have prevented 154 million deaths worldwide, including 146 million in children under five years of age. Thus, they have been responsible for 40% of the reduction in under-five mortality in this period. This reduction has reached 52% in Africa.
Vaccines have been incorporated into routine vaccination programs
Different countries have made major efforts to establish their immunisation programmes. Alongside these, there have also been global health initiatives such as the Expanded Programme on Immunization in 1974 and the Children's Vaccine Initiative in 1991. Gavi (The Vaccine Alliance) was also established in 2000, and the Global Vaccine Action Plan 2011–2020 and the current Immunization Agenda 2030 were published (WHO, 2020)World Health Organization. (2020). Immunization Agenda 2030: A global strategy to leave no one behind. World Health Organization. https://www.who.int/publications/m/item/immunization-agenda-2030-a-global-strategy-to-leave-no-one-behind.
In the first vaccination programs, there were 6 vaccines: tuberculosis, diphtheria, tetanus, pertussis, polio and measles. From that number we have come to have 13 universally recommended vaccines. These include the above plus papilloma, hepatitis B, varicella, pneumococcus, Haemophilus influenzae type B, rotavirus and COVID-19. In addition, there are other 17 more recommended depending on the context, such as those for yellow fever, cholera and meningitis.
All of this led to achieving, in the 1990s, global childhood vaccination coverage of close to 80%, and considerable optimism (Shattock et al., 2024)Shattock, A. J., Johnson, H. C., Sim, S. Y., Carter, A., Lambach, P., Hutubessy, R. C. W., Thompson, K. M., Badizadegan, K., Lambert, B., Ferrari, M. J., Jit, M., Fu, H., Silal, S. P., Hounsell, R. A., White, R. G., Mosser, J. F., Gaythorpe, K. A. M., Trotter, C. L., Lindstrand, A., . . . Bar-Zeev, N. (2024). Contribution of vaccination to improved survival and health: Modelling 50 years of the Expanded Programme on Immunization. The Lancet, 403(10441), 2307–2316. https://doi.org/10.1016/S0140-6736(24)00850-X.
Still, millions of children are not adequately vaccinated
Despite the advances made, it is estimated that each year 7 million newborns fail to receive the complete package of essential vaccines they need. Moreover, a further 13 million children do not receive a single dose (WHO, n.d.)World Health Organization. (n.d.). Immunization dashboard. https://immunizationdata.who.int/.
Today we barely have an overall coverage of 83% for the third dose of diphtheria, tetanus and pertussis (DTP3). Similarly, we barely achieved coverage of 74% for the second dose of measles, or 65% for the third dose of pneumococcus, for example. None of the vaccines introduced in recent years have reached the coverage of the older vaccines. This is despite the fact that some of them have been on the vaccine schedules for more than 10 years.
There are also wide disparities between countries. DTP3 coverage barely reaches 73% in Africa, and 60% of children who had never received any dose of DTP in 2023 live in just ten countries. These are Afghanistan, Angola, DRC, Ethiopia, India, Indonesia, Nigeria, Pakistan, Sudan and Yemen (Geddes, 2024)Geddes, L. (2024, December 6). Charting the unprotected: An illustrated guide to the zero-dose child. VaccinesWork, Gavi. https://www.gavi.org/vaccineswork/charting-unprotected-illustrated-guide-zero-dose-child.
Within a single country there are also differences between rural and urban areas. Likewise, in countries such as India and Afghanistan, vaccination coverage among girls appears to be lower than among boys. In any case, the greatest difference exists according to the wealth and educational level of parents. Indeed, the poorest households are always more exposed and vulnerable. For example, studies suggest there are 27% fewer fully vaccinated children when mothers have had no formal education. A similar gap exists between the poorest and wealthiest quintiles of the population (Ahmed Ali et al., 2022)Ahmed Ali, H., Hartner, A.-M., Echeverria-Londono, S., Roth, J., Li, X., Abbas, K., Portnoy, A., Vynnycky, E., Woodruff, K., Ferguson, N. M., Toor, J., & Gaythorpe, K. A. M. (2022). Vaccine equity in low and middle income countries: A systematic review and meta-analysis. International Journal for Equity in Health, 21, 82. https://doi.org/10.1186/s12939-022-01678-5.
Achieving the "last mile" in vaccination coverage is a major challenge
Today, progress has stalled. In fact, we are still far from the 90% target for coverage for essential childhood vaccines. These include 3 doses of diphtheria, tetanus, pertussis, and pneumococcus, 2 doses of measles, and 1 against papillomavirus.
Reaching that "last mile" from 80% to 90% is of course difficult. In any case, it becomes even more challenging where health systems are weak and have failed to adapt to new demographic patterns. The problem is further compounded when contradictory information or disinformation contributes to reducing public trust in health authorities. Nor can we overlook the impact of the growing number and duration of complex humanitarian crises and conflicts, which pose additional challenges (Aiken et al., 2024)Aiken, D., Richards, H., & Jauset, C. (2024, October). Vaccination barriers in complex settings. MSF Applied Reflection Center for Humanitarian Practice. https://arhp.msf.es/resource/vaccination-barriers-in-complex-settings/.
Alongside the above, since 2020 there has been a setback. This is largely attributable to the indirect effect of the COVID-19 pandemic. In fact, it is believed to be partly the result of redirecting numerous child health resources towards epidemic control. The effect of restrictions and fear of infection on access to health services already strained by the crisis has also carried considerable weight. There were also widespread doubts about the safety of a vaccine developed very rapidly against a disease that many perceived as not particularly serious (Troiano & Nardi, 2021)Troiano, G., & Nardi, A. (2021). Vaccine hesitancy in the era of COVID-19. Public Health, 194, 245–251. https://doi.org/10.1016/j.puhe.2021.02.025. These doubts have affected public confidence in other vaccines.
Vaccine hesitancy is a complex problem that leads to the rejection of vaccines
Vaccine hesitancy refers to the delay in accepting or the outright rejection of vaccination, despite its availability. It represents a significant threat to global health that, although already recognised as such, was exacerbated during the COVID-19 pandemic across very different contexts.
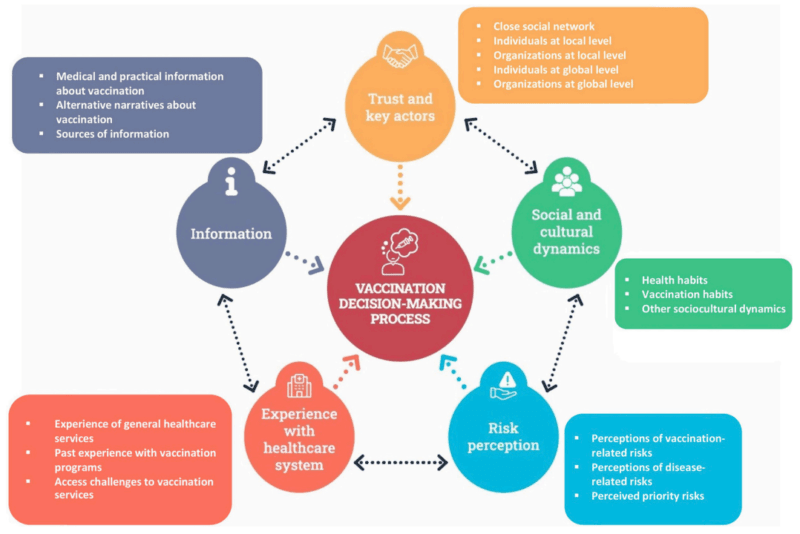
The academic literature on vaccine hesitancy has grown considerably in recent years, producing numerous analyses and conceptual frameworks on the subject. One of them, developed by MSF specialists, proposes a model according to which the decision to get vaccinated or to vaccinate one's children depends on five interrelated factors (Fouqueray et al., 2026)Fouqueray, E., Verschuere, J., Panunzi, I., Bachy, C., & Pellecchia, U. (2026). Addressing the social nature of vaccination hesitancy in humanitarian immunization programs: An experience of developing a qualitative assessment tool on vaccination decision making in Médecins Sans Frontières. Vaccine: X, 30, 100808. https://doi.org/10.1016/j.jvacx.2026.100808:
- The information people have about vaccination and the sources and narratives through which they receive it.
- The trust between individuals and organisations at local and global level.
- Social and cultural dynamics, including habits.
- The perceived risks associated with diseases and with vaccination, with different levels of priority.
- Personal and direct experience with the health system, including vaccination programmes but also other types of health services.
An in-depth analysis of these factors in each context can help to understand the complexity of the problem and the way local populations think. Moreover, through that dialogue, community members can also come to understand the perspective of epidemiological specialists. Only in this way is it possible to grasp the importance of issues that may be critical in some cases, such as the limitations of the health system in managing vaccine side effects, or the trust that community health workers and local staff can provide.
Adapting vaccination strategies and campaigns in humanitarian emergencies
Vaccination campaigns may be necessary in emergencies
Logistical and security challenges are even greater in a humanitarian crisis. These can increase difficulties in the provision of health services or population access to such services, thus reducing vaccination coverage. It is therefore necessary to consider alternatives to health service provision and routine vaccination programs.
One of the most common strategies of vaccination in humanitarian emergencies is to develop mass campaigns in health units or in the community. This is done outside routine vaccination services, which may or may not be operational. The campaigns target expanded age groups, covering only some priority vaccines, and sometimes with reduced schedules. This solution, which in normal situations could be inadequate, is often the most indicated in complex crises. In these circumstances the ideal is far from realistic.
Humanitarian action must, of course, strive to protect and, where possible, support the recovery of the local health system. However, restoring routine vaccination services can take a very long time. In the meantime, actions must be adapted to the urgent needs of the population. Nigeria is a good example of the success of this type of approach. The country had routine vaccination coverage against polio of around 60%. However, emergency vaccination campaigns promoted by the Global Polio Eradication Initiative succeeded in protecting the country from the circulation of wild poliovirus (Nnadi et al., 2017)Nnadi, C., Etsano, A., Uba, B., Ohuabunwo, C., Melton, M., wa Nganda, G., Esapa, L., Bolu, O., Mahoney, F., Vertefeuille, J., Wiesen, E., & Durry, E. (2017). Approaches to vaccination among populations in areas of conflict. The Journal of Infectious Diseases, 216(Suppl. 1), S368–S372. https://doi.org/10.1093/infdis/jix175.
Campaigns of vaccination in humanitarian emergencies should prioritize only certain antigens
To determine which vaccines are priorities, it is recommended to establish a working group led by the Ministry of Health. In its absence, leadership may come from the health cluster. This group of experts will need to (WHO, 2017a)World Health Organization. (2017). Vaccination in acute humanitarian emergencies: A framework for decision making. World Health Organization. https://iris.who.int/handle/10665/255575:
- First assess the epidemiological risks of the different diseases.
- Then analyze the different vaccines available and the possibility of offering them effectively.
- Finally, study other considerations. These include possible barriers and facilitators, as well as viable alternatives to the initial plan. At this stage, the other humanitarian needs competing for scarce resources should also be analyzed.
Analyzing epidemiological risks helps to identify priorities
The first step requires determining the level of risk of each vaccine-preventable disease, due to general and specific risk factors (WHO, 2017a)World Health Organization. (2017). Vaccination in acute humanitarian emergencies: A framework for decision making. World Health Organization. https://iris.who.int/handle/10665/255575. There is no point in prioritising a vaccine for a pathogen that, in a given context, does not pose a health risk.
The analysis should prioritize the potential mortality resulting from the transmission of a disease. In addition, it should assess the pressure on curative health services and the long-term effects of the disease. These include, for example, papillomavirus cervical cancer or vertical transmission of hepatitis B in childbirth. It may also consider the potential setback in global advances in the elimination or eradication of a disease.
The second step is to evaluate the available vaccines
At this stage it is essential to analyse the characteristics of the vaccines and the feasibility of their use (WHO, 2017a)World Health Organization. (2017). Vaccination in acute humanitarian emergencies: A framework for decision making. World Health Organization. https://iris.who.int/handle/10665/255575.
It is necessary to analyze the potential availability of sufficient doses and the recommended administration schedule. In some cases, the possibility of using reduced or even fractionated doses should also be considered. Sometimes it is unrealistic to expect to apply a complete vaccination schedule if the population is on the move or if availability is reduced. The use of a reduced pattern or a fractionated dose tends to generate less durable immunity than usual. However, it may be sufficient to reduce the risk in the most critical period.
The feasibility of vaccination in a given context also depends on other factors. Examples include its presentation (single or multiple doses), its composition, the type of vaccine (attenuated or inactivated), or the cost. In some cases, a determining factor may be the sensitivity of the vaccine to temperatures. The cold chain can be a challenge in remote areas with poor infrastructure. The time it takes for vaccines to generate a protective immune response against pathogens is also a determining factor. Attenuated vaccines can provide sufficient protection with only one or two doses in as little as two weeks. However, inactivated vaccines require more doses, spaced several weeks apart, to provide a similar level of protection. Similarly, depending on the time of year or seasonal risk of certain diseases, some vaccines may be prioritized and others postponed.
Possible vaccination strategies should also be evaluated
Factors such as the difficulty of accessing certain geographical areas and populations can be decisive. It is also necessary to consider whether a fixed-post strategy (at health centres, schools, churches, mosques or markets) or mobile teams would be more appropriate. This is important, for example, for nomadic populations without access to a fixed vaccination post. Sometimes it may be necessary to combine both approaches. In other cases, however, it may also be feasible to attempt to restore routine vaccination services from the outset. It is also essential to assess whether there are sufficient staff and material resources, such as means of transport, fuel or refrigerators, to reach the target population (WHO, 2017b)World Health Organization. (2017). Vaccination in acute humanitarian emergencies: Implementation guide. World Health Organization. https://www.who.int/publications/i/item/WHO-IVB-17.13.
A key factor is whether it is possible to ensure adequate information and awareness-raising among the population about vaccines within the limited time available. For this, social mobilisation is always essential (Ismail et al., 2022)Ismail, S. A., Lam, S. T., Bell, S., Fouad, F. M., Blanchet, K., & Borghi, J. (2022). Strengthening vaccination delivery system resilience in the context of protracted humanitarian crisis: A realist-informed systematic review. BMC Health Services Research, 22, 1277. https://doi.org/10.1186/s12913-022-08653-4. It is important to use multiple channels, from mass media to traditional and religious leaders and community health workers. It is also essential to understand the doubts and perceptions of the population regarding the risk of contagion and their views on vaccines. This allows messages and the way they are communicated to be properly adapted.
Despite the importance of this dialogue, in emergencies and partly due to logistical difficulties, difficult decisions sometimes have to be made. In some cases informed consent may be limited to verbal consent. In exceptional cases of serious public health emergencies, authorities could even determine that vaccination is mandatory. However, both of these situations can give rise to significant ethical dilemmas.
In the third step, other considerations and possible dilemmas are discussed
The third and final step in decision-making on vaccination in humanitarian emergencies is based on the analysis of ethical and political considerations. Security aspects, other concurrent needs to be considered, and contextual factors that may pose barriers to vaccination must all be assessed (WHO, 2017a)World Health Organization. (2017). Vaccination in acute humanitarian emergencies: A framework for decision making. World Health Organization. https://iris.who.int/handle/10665/255575.
From an ethical standpoint, it is often not easy to decide that a vaccination campaign will leave certain lower-risk groups unprotected (Moodley et al., 2013)Moodley, K., Hardie, K., Selgelid, M. J., Waldman, R. J., Strebel, P., Rees, H., & Durrheim, D. N. (2013). Ethical considerations for vaccination programmes in acute humanitarian emergencies. Bulletin of the World Health Organization, 91(4), 290–297. https://doi.org/10.2471/BLT.12.113480. After all, they have the same rights. It is equally difficult to balance the importance of community participation in decision-making with the need for rapid action. Furthermore, the insecurity of the population and of health staff in conflict zones is always an aspect to be considered and managed.
Finally, we cannot forget the ongoing humanitarian dilemma of having to prioritize some interventions or populations over others. The reason is clear: there are never enough resources for everything. Sometimes, starting a vaccination campaign against a pathogen can consume resources that could be used for other health problems. Likewise, opting for some vaccines and not others will benefit some people and harm (or not benefit) others.
Not all decisions about vaccination in humanitarian emergencies are made according to technical criteria
Although the three decision-making steps appear logical, reality rarely allows them to be followed in full. In most crises, a very limited number of diseases are prioritised in vaccination campaigns (such as measles or polio) (Leach & Checchi, 2022)Leach, K., & Checchi, F. (2022). The utilisation of vaccines in humanitarian crises, 2015–2019: A review of practice. Vaccine, 40(21), 2970–2978. https://doi.org/10.1016/j.vaccine.2022.03.034. This is the case despite the high risk of HPV due to high rates of sexual and gender-based violence (Allison et al., 2023)Allison, L. E., Alhaffar, M., Checchi, F., Abdelmagid, N., Nor, B., Sabahelzain, M. M., Light, P. M., & Singh, N. S. (2023). A systematic review of vaccination guidance for humanitarian responses. Vaccines, 11(12), 1743. https://doi.org/10.3390/vaccines11121743, or the high risk of rotavirus due to poor water, sanitation and hygiene conditions. Even when an expert panel has offered a coherent recommendation, authorities often make decisions based on other criteria.
🧠 Let's pause and reflect
Why do decisions about which vaccines to prioritise in humanitarian emergencies not always follow technical criteria, and what are the consequences of this?
- 1Think and write your answer.
- 2Click on «Copy and open».
- 3Paste to receive feedback.
📚 This is the NotebookLM for this topic. It uses only carefully selected references. | What is NotebookLM?
Gavi, COVAX and other global initiatives for access to vaccines in emergencies
Many initiatives try to cope with the high cost of vaccines
The high cost of vaccines is, of course, a major constraint. In the face of this, some global initiatives have emerged, such as Gavi (the Vaccine Alliance), the Humanitarian Mechanism, or COVAX.
Gavi is a public-private partnership created with the aim of providing more than 20 different vaccines at affordable prices to low- and middle-income countries. The Humanitarian Mechanism, however, is a collaboration between MSF, Save the Children, UNICEF and the WHO (WHO et al., 2021)WHO, UNICEF, MSF, & Save the Children. (2021, March 4). Accessing affordable and timely supply of vaccines for use in humanitarian emergencies: The Humanitarian Mechanism – WHO working document. World Health Organization. https://cdn.who.int/media/docs/default-source/immunization/the-humanitarian-mechanism-tors.pdf. This alliance of humanitarian actors seeks to negotiate reduced prices with major pharmaceutical companies for vaccines such as the pneumococcal vaccine. Without discounts, their use by humanitarian organisations in emergencies can be impossible. Finally, COVAX was an initiative developed between 2020 and 2023 in response to the COVID-19 pandemic. It sought to facilitate access to vaccines against this disease for low- and middle-income countries, though with insufficient results (MSF Access, 2021)MSF Access. (2021, December 21). COVAX: A broken promise to the world – Issue brief. Médecins Sans Frontières. https://msfaccess.org/covax-broken-promise-world.
A global stockpile of vaccines is available for use in epidemics
On occasion, the challenge of insufficient access to vaccines in a country arises not for prevention purposes, but for epidemic control. This is because in many fragile contexts there are not enough vaccines for the control of large infectious disease outbreaks.
For this reason, in 1997 the WHO, UNICEF, IFRC and MSF founded the International Coordination Group on Vaccine Provision (WHO, 2019)World Health Organization. (2019). Reform of the International Coordinating Group for Vaccine Provision: A new framework for coordination, accountability and transparency. Weekly Epidemiological Record, 94(49), 591–600. https://iris.who.int/bitstream/handle/10665/330046/WER9449-591-600-eng-fre.pdf. Since then, this body has progressively improved its governance and accountability. It has also succeeded in consolidating its funding with the support of Gavi (The Vaccine Alliance). Today this mechanism maintains a global emergency stock of vaccines for meningitis, yellow fever, cholera and Ebola. This reserve can be distributed immediately in the event of major epidemics. To date, it has distributed more than 250 million doses (WHO, 2026)World Health Organization. (2026). About the International Coordinating Group (ICG) on Vaccine Provision. https://www.who.int/groups/icg/about.

This group, however, depends in turn on collaboration with pharmaceutical companies for the manufacture of vaccines. It also depends on UNICEF for the distribution of doses.
In addition, it collaborates with national governments (and their partners) on vaccination interventions. This includes the detection and confirmation of outbreaks, the dispatch of requests and the management of incoming vaccines. The latter starts with customs procedures for entry into the country. It continues with the maintenance of their cold chain during storage and transport domestically, and ends with the development of vaccination campaigns.
References
- Ahmed Ali, H., Hartner, A.-M., Echeverria-Londono, S., Roth, J., Li, X., Abbas, K., Portnoy, A., Vynnycky, E., Woodruff, K., Ferguson, N. M., Toor, J., & Gaythorpe, K. A. M. (2022). Vaccine equity in low and middle income countries: A systematic review and meta-analysis. International Journal for Equity in Health, 21, 82. https://doi.org/10.1186/s12939-022-01678-5
- Aiken, D., Richards, H., & Jauset, C. (2024, October). Vaccination barriers in complex settings. MSF Applied Reflection Center for Humanitarian Practice. https://arhp.msf.es/resource/vaccination-barriers-in-complex-settings/
- Allison, L. E., Alhaffar, M., Checchi, F., Abdelmagid, N., Nor, B., Sabahelzain, M. M., Light, P. M., & Singh, N. S. (2023). A systematic review of vaccination guidance for humanitarian responses. Vaccines, 11(12), 1743. https://doi.org/10.3390/vaccines11121743
- Fouqueray, E., Verschuere, J., Panunzi, I., Bachy, C., & Pellecchia, U. (2026). Addressing the social nature of vaccination hesitancy in humanitarian immunization programs: An experience of developing a qualitative assessment tool on vaccination decision making in Médecins Sans Frontières. Vaccine: X, 30, 100808. https://doi.org/10.1016/j.jvacx.2026.100808
- Geddes, L. (2024, December 6). Charting the unprotected: An illustrated guide to the zero-dose child. VaccinesWork, Gavi. https://www.gavi.org/vaccineswork/charting-unprotected-illustrated-guide-zero-dose-child
- Ismail, S. A., Lam, S. T., Bell, S., Fouad, F. M., Blanchet, K., & Borghi, J. (2022). Strengthening vaccination delivery system resilience in the context of protracted humanitarian crisis: A realist-informed systematic review. BMC Health Services Research, 22, 1277. https://doi.org/10.1186/s12913-022-08653-4
- Leach, K., & Checchi, F. (2022). The utilisation of vaccines in humanitarian crises, 2015–2019: A review of practice. Vaccine, 40(21), 2970–2978. https://doi.org/10.1016/j.vaccine.2022.03.034
- Moodley, K., Hardie, K., Selgelid, M. J., Waldman, R. J., Strebel, P., Rees, H., & Durrheim, D. N. (2013). Ethical considerations for vaccination programmes in acute humanitarian emergencies. Bulletin of the World Health Organization, 91(4), 290–297. https://doi.org/10.2471/BLT.12.113480
MSF Access. (2021, December 21). COVAX: A broken promise to the world [Issue brief]. Médecins Sans Frontières. https://msfaccess.org/covax-broken-promise-world
- Nnadi, C., Etsano, A., Uba, B., Ohuabunwo, C., Melton, M., wa Nganda, G., Esapa, L., Bolu, O., Mahoney, F., Vertefeuille, J., Wiesen, E., & Durry, E. (2017). Approaches to vaccination among populations in areas of conflict. The Journal of Infectious Diseases, 216(Suppl. 1), S368–S372. https://doi.org/10.1093/infdis/jix175
- Shattock, A. J., Johnson, H. C., Sim, S. Y., Carter, A., Lambach, P., Hutubessy, R. C. W., Thompson, K. M., Badizadegan, K., Lambert, B., Ferrari, M. J., Jit, M., Fu, H., Silal, S. P., Hounsell, R. A., White, R. G., Mosser, J. F., Gaythorpe, K. A. M., Trotter, C. L., Lindstrand, A., . . . Bar-Zeev, N. (2024). Contribution of vaccination to improved survival and health: Modelling 50 years of the Expanded Programme on Immunization. The Lancet, 403(10441), 2307–2316. https://doi.org/10.1016/S0140-6736(24)00850-X
- Troiano, G., & Nardi, A. (2021). Vaccine hesitancy in the era of COVID-19. Public Health, 194, 245–251. https://doi.org/10.1016/j.puhe.2021.02.025
- WHO, UNICEF, MSF, & Save the Children. (2021, March 4). Accessing affordable and timely supply of vaccines for use in humanitarian emergencies: The Humanitarian Mechanism [WHO working document]. World Health Organization. https://cdn.who.int/media/docs/default-source/immunization/the-humanitarian-mechanism-tors.pdf
- World Health Organization. (2017a). Vaccination in acute humanitarian emergencies: A framework for decision making. World Health Organization. https://iris.who.int/handle/10665/255575
- World Health Organization. (2017b). Vaccination in acute humanitarian emergencies: Implementation guide. World Health Organization. https://www.who.int/publications/i/item/WHO-IVB-17.13
- World Health Organization. (2019). Reform of the International Coordinating Group for Vaccine Provision: A new framework for coordination, accountability and transparency. Weekly Epidemiological Record, 94(49), 591–600. https://iris.who.int/bitstream/handle/10665/330046/WER9449-591-600-eng-fre.pdf
- World Health Organization. (2020). Immunization Agenda 2030: A global strategy to leave no one behind. World Health Organization. https://www.who.int/publications/m/item/immunization-agenda-2030-a-global-strategy-to-leave-no-one-behind
- World Health Organization. (2022). A brief history of vaccination. https://www.who.int/news-room/spotlight/history-of-vaccination/a-brief-history-of-vaccination
- World Health Organization. (2026). About the International Coordinating Group (ICG) on Vaccine Provision. https://www.who.int/groups/icg/about
- World Health Organization. (n.d.). Immunization dashboard. https://immunizationdata.who.int/
- The 21st Century and the resurgence of infections
- International public health emergencies
- Diarrheal diseases and cholera
- Tuberculosis and pneumonia: respiratory infections
- Malaria: progress and challenges toward elimination
- Vaccination in humanitarian emergencies
- Response to epidemics in humanitarian crises
NotebookLM
You can review my literature references on vaccination in humanitarian emergencies with this NotebookLM, an artificial intelligence-based research assistant. Do you want to know more?
How to cite this page
Abarca, B. (June 29, 2026). Vaccination in humanitarian emergencies: coverage, campaigns and access to vaccines. Salud Everywhere. https://saludeverywhere.com/en/health-in-humanitarian-crises/vaccination-in-humanitarian-emergencies/