Attacks on aid workers and health care: data, causes and protection
- Page updated onJuly 16, 2026

Attacks on aid workers and health care have reached record highs. In 2025, the more than 700 incidents of violence against aid workers left nearly 1,200 victims among those killed, injured, kidnapped and detained, and health workers were exposed to over 2,500 attacks in countries in conflict. Most of the victims are national staff, and increasingly the perpetrator of these attacks is a state actor.
This page examines the data, causes and international responses to this form of violence, directed against those who provide aid to civilians and people in need of humanitarian assistance.
Table of contents:
What is the scale of violence against aid workers?
How has violence against aid workers evolved over the past thirty years?
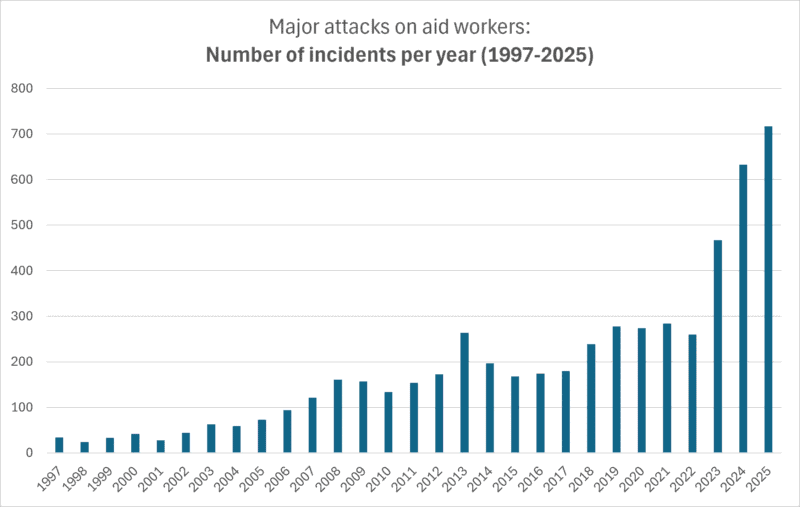
Thanks to several global initiatives to record and verify serious incidents of violence and detention against aid workers, such as the Aid Worker Security Database (AWSD), we now know that the figures have kept rising (Humanitarian Outcomes, n.d.). In fact, 2025 saw record highs, with 710 reported incidents affecting 1,185 humanitarian professionals (according to provisional figures as of 15 July 2026).
1997 is the earliest year for which reliable figures exist on violent incidents and affected aid workers, according to the analyses that began in 2005 (Stoddard et al., 2006). Since then, the number of incidents has doubled or tripled decade on decade. While 34 violent incidents were recorded in 1997, 710 were recorded in 2025, some 21 times more.
The analysis of the data between 1997 and 2005 revealed that much of the increase in the number of violent incidents against aid workers reflected the growth of the humanitarian system (Stoddard et al., 2006). Even as security management systems improved and increasingly restrictive practices were adopted in humanitarian operations, humanitarian funding grew, and with it the deployment of staff exposed to attacks.
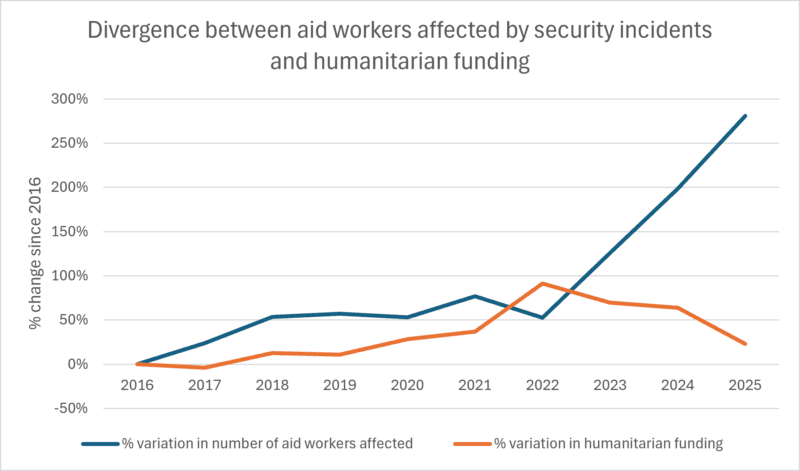
However, if we cross-reference the humanitarian funding data from OCHA's Financial Tracking Service with the figures on aid workers affected by violent incidents, we see that at a certain point the trend changes sharply. From 2022 onwards, attacks on aid workers rise far more steeply than in previous years, while humanitarian funding falls. In 2025, the global volume of humanitarian funding drops to levels close to those of 2016, while the number of aid workers affected by security incidents is 281% higher (Humanitarian Outcomes, n.d.).
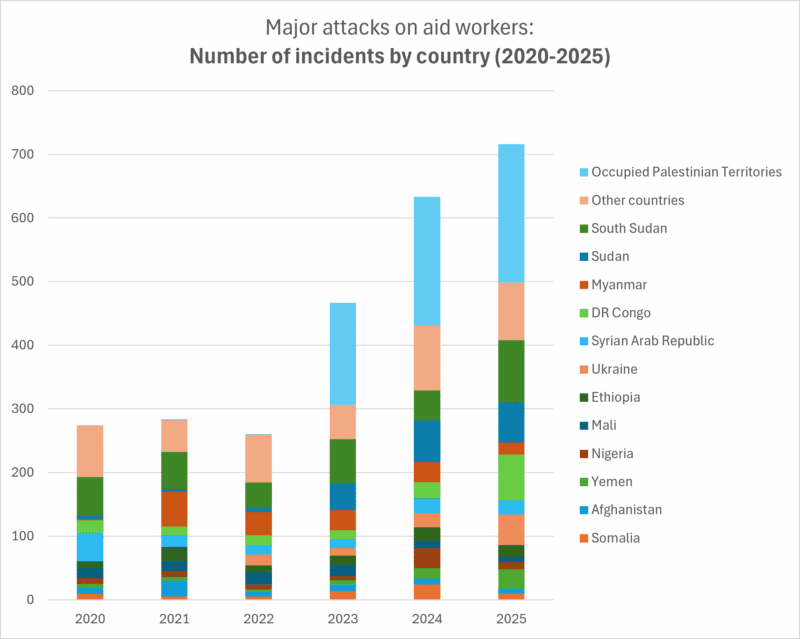
The analysis of violent-incident data by country helps explain this divergence. Their geographical distribution varies year on year, depending on the severity of the humanitarian crises and the political context in which they occur. However, from 2023 onwards attacks targeting aid workers in the Occupied Palestinian Territories rise sharply, far above any other country.
In 2025, of the 710 recorded security incidents, 212 occurred in the Occupied Palestinian Territories. The next countries with the most incidents were South Sudan (97), the Democratic Republic of the Congo (72), Sudan (63) and Ukraine (47) (Humanitarian Outcomes, n.d.).
Who are the victims?: mostly national aid workers
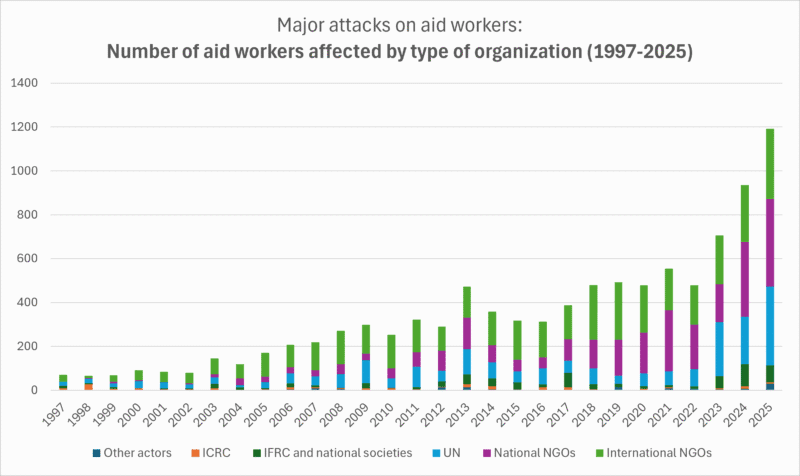
Over the years, most of the victims of attacks and security incidents have been aid workers in NGOs, both international and national, followed by the United Nations. Attacks affecting staff of the International Red Cross and Red Crescent Movement and the National Societies are also significant. In 2025, however, of the 1,185 aid workers affected by violent incidents, 396 worked for national NGOs, 363 for the United Nations, 319 for international NGOs, and 78 for the International Red Cross and Red Crescent Movement (Humanitarian Outcomes, n.d.).
It is important to understand that the Aid Worker Security Database counts as aid workers the employees and volunteers of not-for-profit humanitarian agencies, such as the Red Cross and Red Crescent, NGOs, UN humanitarian agencies, donors and other organisations whose activities are considered humanitarian. It does not include, however, United Nations peacekeeping personnel, human rights defenders, electoral observers, or purely religious, political or activist organisations. Nor does it include health system staff unless they receive direct or indirect support from humanitarian organisations (Humanitarian Outcomes, 2026b).
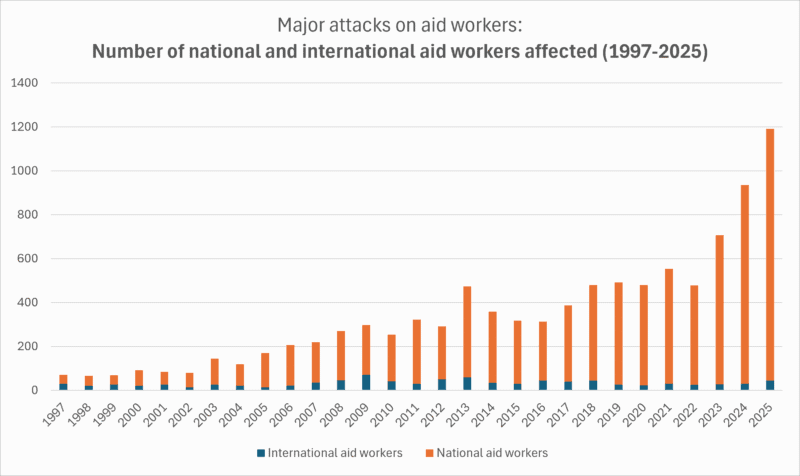
The victims are, for the most part, national aid workers, not international expatriate staff. All humanitarian organisations have far more national than international staff in the countries where they operate, and it is national staff who are most exposed to threats and attacks.
In 2025, 1,141 national and 44 international aid workers were victims of violent incidents (Humanitarian Outcomes, n.d.).
What kinds of security incidents occur and what do they result in?
Not all attacks are the same, and neither are their outcomes. There are deaths, kidnappings lasting more than 24 hours, serious wounds and injuries requiring medical treatment, and detentions or arrests lasting more than 24 hours (Humanitarian Outcomes, 2026b). In fact, although the first three have historically been the main ones, since 2023 the detention of aid workers by authorities has emerged as an incident type — without formal charges, a clear timeframe or established conditions for their release.
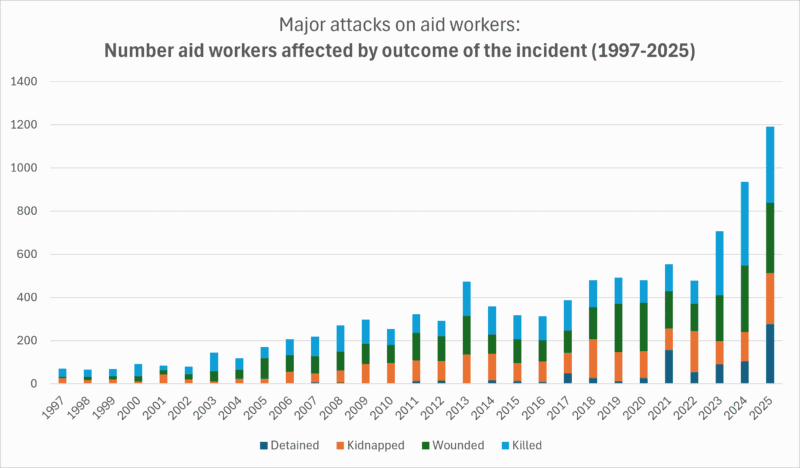
In 2025, 350 aid workers died as a result of attacks and security incidents and 322 suffered wounds and injuries requiring medical care. 278 were detained without formal charges for more than 24 hours and 235 were kidnapped or abducted (Humanitarian Outcomes, n.d.):
- Most of the deaths (53%) were concentrated in the Occupied Palestinian Territories, and especially in Gaza, followed by Sudan (20%). Most deaths resulted from bombing and missile and drone strikes, followed by shootings. In many cases the victims were in clearly identified humanitarian vehicles and facilities, wearing visible humanitarian vests, as well as in hospitals and clinics run or supported by humanitarian actors. In other cases, staff were killed off duty, at home and alongside their families, in air strikes.
- Most aid workers who were injured were so as a result of air, missile and drone strikes. In certain contexts such as Sudan or the Democratic Republic of the Congo, however, gunshot wounds were very common, in robberies, crossfire and ambushes on vehicles. Numerous cases of stabbings and beatings are also recorded.
- Detentions, far from being brief holds at routine checkpoints, have emerged since 2023 as the way in which state power exerts violence against humanitarian action through seemingly legal means, based on accusations of espionage or breaches of administrative requirements that criminalise it (Humanitarian Outcomes, 2026a), mainly in Yemen, South Sudan and the Democratic Republic of the Congo. Although many cases are resolved within a few days, this category also includes long-term detentions.
- As for kidnappings, most cases were carried out by non-state armed groups in the Democratic Republic of the Congo, Sudan, South Sudan or Ethiopia, and ended in release after several hours or days. Some, however, result in prolonged captivity and disappearances with unknown whereabouts. They occur not only for economic reasons, but also to exert and contest territorial control, or on suspicion of collaboration with the enemy. In some cases, the trigger was precisely being clearly identified as aid or health workers. In Pakistan, for example, there were several cases of polio vaccinators being kidnapped.
The perpetrators of the violence
Since 2023, the main perpetrator of violent incidents against aid workers has been the host state and its military, police and security forces. Setting aside the cases of unknown authorship, they are followed by non-state armed groups and, in third place, foreign or coalition forces (Humanitarian Outcomes, n.d.).
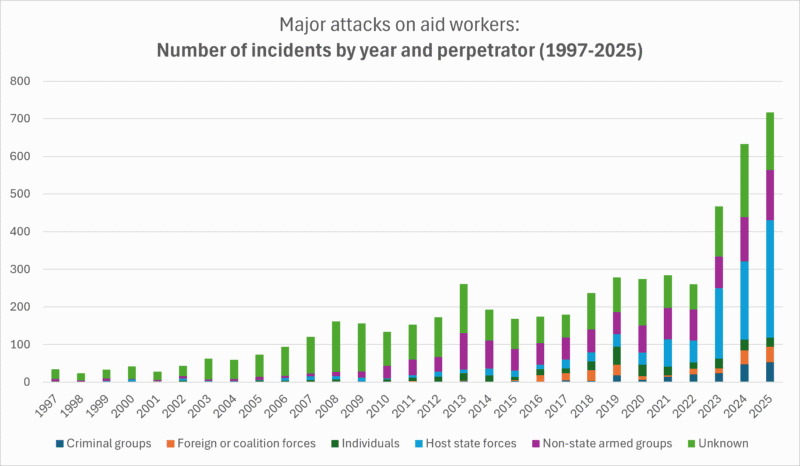
This state prominence is overwhelmingly concentrated in the Occupied Palestinian Territories, where 60% of all incidents attributed to host states between 2023 and 2025 took place (Humanitarian Outcomes, n.d.).
Funding cuts increase vulnerability to attacks, and both lead to the closure of humanitarian operations
The vulnerability of humanitarian organisations and their staff to attacks has increased since 2025, as a result of cuts in humanitarian funding. Reducing contributions cuts the resources available for logistics, transport, coordination and security risk management. Programmes are also interrupted or cancelled, which can breed resentment among the local population and even reprisals from armed groups (Stoddard et al., 2025).
Violent incidents also have a clear and documented impact on the shrinking of humanitarian space and dramatic consequences for people in need of assistance. Projects are closed and interrupted, less effective modes of delivering assistance have to be adopted, and barriers are imposed on the provision of goods essential for survival (Hilhorst & Jansen, 2010).
What are attacks on health care and how do they differ?
There is a phenomenon that, unfortunately, coexists and overlaps with violence against aid workers: attacks directed at health workers in armed conflict. The WHO defines them as any act of physical or verbal violence, threat of violence, psychological violence or obstruction that interferes with the availability, access to and delivery of health services, curative or preventive (WHO, 2019).
Scale and trends of attacks on health care in humanitarian crises
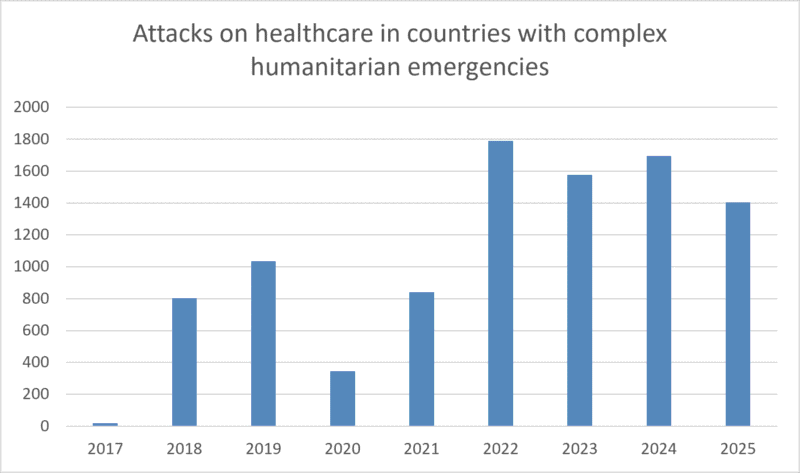
In 2012, the World Health Assembly, recognising the need for systematic data collection on attacks against medical missions, health workers and users of health services in armed conflict, mandated the WHO to document them (World Health Assembly, 2012). Five years later, in 2017, the Surveillance System for Attacks on Health Care (SSA) was officially launched (WHO, n.d.).
In 2017 the record was still partial, in 2020 the COVID-19 pandemic reduced data-collection capacity, and there is likely significant under-reporting. In any case, this WHO system shows that since 2022 there have been between 1,400 and 1,800 attacks each year against health workers and services in countries with complex humanitarian emergencies (WHO, n.d.).
On the other hand, the Safeguarding Health in Conflict Coalition (SHCC) was founded in 2011, made up of some 40 organisations united to raise awareness of attacks, strengthen their documentation and advocate for the right to health. According to this coalition's data, which uses a broader methodology than the WHO and covers more countries, in 2025 there were 2,546 violent incidents against health services in 33 countries in conflict. 790 hospitals or health centres were damaged or destroyed, 455 professionals were killed, 218 were kidnapped and 263 were detained (SHCC & Insecurity Insight, 2026).
Are there more than before? Have they increased? Is this a new normal? These questions are hard to answer. What is clear is that, although attacks today are more visible and better documented, there is also evidence that violence against health care in conflict has always existed (Rubenstein, 2021).
Why are those who provide aid attacked?
Aid and health workers are often targeted for similar reasons, such as operating in the same contexts and assisting all those in need with neutrality and impartiality. This, which ought to protect them, is precisely what exposes them to violence.
Understanding the interests and incentives of the perpetrators of violent incidents, and the specific differences in the case of attacks on health workers — who are specially protected by International Humanitarian Law and have been for years (Bernard, 2013) — is essential to understanding how to mitigate the risks.
What are the motives of the perpetrators of violence against aid workers?
The Aid Worker Security Database records three types of motive: political, economic and incidental (Stoddard et al., 2017).
- A political motive aligns with the political ambitions of a group, whether state or non-state. These ambitions may relate to delegitimising and destabilising the enemy, or even to demonstrating strength and subjugating the local population. Sometimes aid workers are not the main target, but attacking them is a means of harming their opponents or the local population.
- The economic motive relates to the theft of money and goods, as well as to the collection of ransoms for kidnappings.
- The incidental category applies when the aid worker is the victim of attacks that, at least as far as can be established, were not directed at them.
In the case of state actors, they often act violently shielded by an atmosphere of impunity. This is, at least in part, the result of the lack of legal and political consequences for the attacks or the continued breach of International Humanitarian Law (Stoddard et al., 2017).
The logic of attacks on health workers and services in humanitarian crises
Attacks on health care in complex humanitarian crises may occur for reasons that overlap with those of attacks on humanitarian actors of all kinds, but they also follow patterns with a specific, multi-dimensional logic (Rubenstein, 2021):
- Attacks to deny health care to wounded and sick people regarded as the enemy or as linked to the enemy. This logic is also followed when it is perceived that these people, whether combatants or civilians, may be using health facilities as a refuge.
- Threats and attacks to destroy or reduce access to health care for entire populations. It is a form of collective punishment sometimes used against populations accused of supporting the opponent, to intimidate them or to force their displacement.
- Attacks to gain tactical advantage. This happens when attackers use confiscated or stolen vehicles to transport weapons and soldiers, health facilities as infrastructure from which to launch attacks, and medical supplies to fund other military actions or to treat their own combatants, going as far as kidnapping the health workers themselves to that end.
- Attacks of convenience, failing to take precautions to protect the wounded, the sick and their carers. These precautions are mandatory, but they are avoided on pretexts of military interest, such as denying the transport of the sick through checkpoints. This is also the logic used when attacking hospitals suspected of sheltering enemy armed groups, without warnings or measures to minimise possible harm to patients and health workers.
- Attacks to express discontent with the quality and organisation of health services or with the authorities that govern them. This is sometimes combined with the spread of disinformation and conspiracy theories, but it may also stem from communities' fear or anger. This type of violence, unlike the previous ones, does not come from the parties to the conflict and has been seen, for example, during the response to the COVID-19 pandemic.
What is being done to protect them?
Over the years, more attention has been paid to attacks on aid and health workers in complex humanitarian crises. The creation of databases such as the Aid Worker Security Database or the WHO Surveillance System for Attacks on Health Care has made it possible to gauge the scale of the incidents and understand their typology: causes, outcomes, people affected and perpetrators. Other organisations have also made major contributions to this body of evidence in defence of the right to health (Human Rights Watch, 2026).
In parallel, humanitarian organisations have not only used this information for advocacy, through campaigns demanding that aid and health workers not be a target of attacks, or initiatives such as Health Care in Danger (ICRC, n.d.). They have also been forced to strengthen their security and risk-reduction measures and, at times, to interrupt highly necessary humanitarian action.
Important United Nations Security Council resolutions have also been passed, such as 2286 (UN Security Council, 2016). It recalls the mandatory compliance with International Humanitarian Law regarding the distinction between combatants and civilians, the prohibition on carrying out indiscriminate attacks and the obligation to take precautionary measures to minimise harm. The resolution also condemns attacks and threats against the wounded, the sick, health workers and health facilities, and calls for accountability and an end to impunity, urging Member States to conduct independent investigations.
However, 10 years after the publication of Resolution 2286, violence, far from receding, has intensified. Although the laws are in place, the political will and leadership are lacking to translate the commitments into concrete action, to ensure accountability and to end violence against health and aid workers (Rubenstein et al., 2025).
References
- Bernard, V. (2013). Editorial: Violence against health care: Giving in is not an option. International Review of the Red Cross, 95(889), 5–12. https://doi.org/10.1017/S1816383114000125
- Hilhorst, D., & Jansen, B. J. (2010). Humanitarian space as arena: A perspective on the everyday politics of aid. Development and Change, 41(6), 1117–1139. https://doi.org/10.1111/j.1467-7660.2010.01673.x
- Human Rights Watch. (2026, May 28). Attacks on health. https://www.hrw.org/feature/2026/05/28/attacks-on-health
- Humanitarian Outcomes. (2026a). Aid Worker Security and the Risk of State Detentions [Video]. YouTube. https://www.youtube.com/watch?v=lvuO8sF-8OY
- Humanitarian Outcomes. (2026b). Aid Worker Security Database codebook. https://humanitarianoutcomes.org/AWSD-codebook
- Humanitarian Outcomes. (n.d.). Aid Worker Security Database. Retrieved July 15, 2026, from https://www.aidworkersecurity.org/
- International Committee of the Red Cross. (n.d.). Health Care in Danger. Retrieved July 16, 2026, from https://healthcareindanger.org/
- Rubenstein, L. (2021). Perilous medicine: The struggle to protect health care from the violence of war. Columbia University Press. https://cup.columbia.edu/book/perilous-medicine/9780231192460/
- Rubenstein, L., Haar, R. J., & Amon, J. J. (2025). Attacks on healthcare in war are being steadily normalized—we need to end impunity. BMJ, 390, r1964. https://doi.org/10.1136/bmj.r1964
- Safeguarding Health in Conflict Coalition, & Insecurity Insight. (2026). Care in the crosshairs: Violence against health care in conflict 2025. https://www.insecurityinsight.org/wp-content/uploads/2026/04/2025-SHCC-Annual-Report.pdf
- Stoddard, A., Breckenridge, M.-J., Czwarno, M., & Duque-Díez, M. (2025). Aid Worker Security Report 2025 — Defenceless: Aid worker security amid the humanitarian funding collapse. Humanitarian Outcomes. https://humanitarianoutcomes.org/AWSR_2025
- Stoddard, A., Harmer, A., & Haver, K. (2006). Providing aid in insecure environments: Trends in policy and operations (HPG Report 23). Humanitarian Policy Group, Overseas Development Institute. https://humanitarianoutcomes.org/sites/default/files/publications/providingaidininsecureenvironments-full.pdf
- Stoddard, A., Harmer, A., & Czwarno, M. (2017). Aid worker security report 2017 — Behind the attacks: A look at the perpetrators of violence against aid workers. Humanitarian Outcomes. https://humanitarianoutcomes.org/publications/aid-worker-security-report-2017-behind-attacks-look-perpetrators-violence-against-aid
- United Nations Security Council. (2016). Resolution 2286 (2016) (S/RES/2286). https://docs.un.org/en/S/RES/2286(2016)
- World Health Assembly. (2012). WHO’s response, and role as the health cluster lead, in meeting the growing demands of health in humanitarian emergencies (Resolution WHA65.20). https://iris.who.int/server/api/core/bitstreams/7b0ecd72-d7e6-4c32-a41c-ad3a48021324/content
- World Health Organization. (2019). Surveillance system for attacks on health care (SSA): Methodology, Version 1.0. https://www.who.int/publications/i/item/surveillance-system-for-attacks-on-health-care-(-ssa)
- World Health Organization. (n.d.). Surveillance System for Attacks on Health Care (SSA) [Database]. Retrieved July 16, 2026, from https://extranet.who.int/ssa/Index.aspx
NotebookLM
You can review my bibliographic references on attacks on aid workers and health care with this NotebookLM, an AI-based research assistant. Want to know more?
How to cite this page
Abarca, B. (17 de July de 2026). Attacks on aid workers and health care: data, causes and protection. Salud Everywhere. https://saludeverywhere.com/en/humanitarian-aid-and-international-development/attacks-aid-workers-health-care/