Maternal and newborn health in humanitarian settings: history, mortality, EmONC and maternal well-being
- Page updated onJune 29, 2026

Maternal and newborn health today occupies a central place in the global sustainable development agenda and in humanitarian priorities, but this was not always the case. In the past, it was a forgotten issue that, along with the other aspects linked to reproductive health and rights, remained in the shadows of other public health priorities.
Fortunately, significant progress has already been made in reducing maternal and neonatal mortality, but there are still profound inequities that (as is almost always the case) go hand in hand with conflicts and humanitarian crises. Therefore, we must defend the importance of emergency obstetric and neonatal care and the relevance of protecting maternal well-being, an aspect that becomes a priority where survival is almost achieved.
Table of contents:
History and evolution of maternal and newborn health in public health and global health policies.
Maternal mortality in the 1980s: from neglect to a Safe Motherhood Initiative with major gaps
In 1985, Deborah Maine and Allan Rosenfield posed an uncomfortable question to the world: Why doesn't maternal mortality get the attention it deserves? At the time, figures of 100-300 maternal deaths per 100,000 births were commonplace in many countries. The question pointed to the neglect of women and was driven by the feminism of the previous years. It came when the Primary Health Care strategy was still in its infancy, and barely focused on child health: diarrhea, malnutrition and respiratory diseases. Maternal health was barely considered from the demographic interest in family planning and preventive prenatal care services. In the background were childbirth care and the main causes of the 500,000 maternal deaths that occurred annually.
Just two years later, in 1987, WHO, UNFPA and the World Bank launched an international conference in Nairobi, which was to be the seed for the Safe Motherhood Initiative. This new interest in reducing maternal mortality carried over into discussions at conferences and societies around the world and helped to look beyond child health and family planning. Interest in prenatal care and gender equity now increased, which was undoubtedly positive, but the focus on reducing maternal deaths was still diffuse.
On the one hand, it was still erroneously believed that both socioeconomic development in general and prevention through early detection of problems in prenatal care were sufficient. This is not the case. Although both are desirable, most obstetric complications are neither easily predictable nor preventable. The key is in their management, and that requires emergency obstetric care, accessible in the community.
Towards the Millennium Development Goals and maternal mortality reduction
In the 1990s, the Cairo and Beijing conferences contributed, among other things, to putting the focus on safe motherhood within a broader framework of reproductive and women's health, finally understood as a human right. This, which today may seem obvious, also generated discomfort for many actors willing to support childbirth care, but not so willing to facilitate contraception or abortion in an ambivalence that, unfortunately, still persists.
As a result of all these changes and advances, maternal health was included in a privileged place among the health and development priorities of the Millennium Development Goals. At last, the world and political authorities were facing a clear goal of global health: reduce maternal mortality by 75%. Moreover, by that time there was already a large evidence base of what worked and what didn't. It was not enough to train traditional birth attendants or facilitate access to prenatal care. There was a need for strong health systems that put women's health during pregnancy and childbirth at the center of their priorities, so that life-threatening obstetric complications could be addressed.
The years 2010 and 2020: uneven progress in maternal mortality reduction
Committing to the Millennium Development Goals had a clear effect. Between 2000 and 2023 maternal mortality fell by 40%, from 328 to 197 deaths per 100,000 live births. However, it is still almost triple the target of 70, proposed for 2030. Moreover, the improvement appears to be stalling. Moreover, as is often the case in global health, the average value hides horrible inequities.
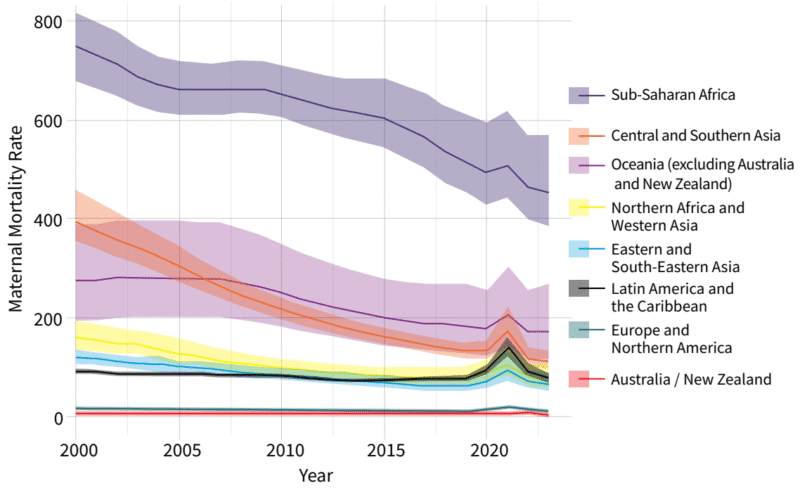
The maternal mortality rate in sub-Saharan Africa remains above 400 per 100,000 live births. Once again, health inequity follows economic inequalities and humanitarian crises. While, in high-income countries, the maternal mortality rate is around 11 per 100,000 births, in low-income countries it reaches 421 deaths and in conflict-affected countries, 504; fifty times more.
In addition, maternal mortality has not been reduced at the same rate as the coverage of childbirth care has increased. This exposes a serious problem in the quality of health services. Although 75% of women have had a birth attended by a skilled professional and more than two-thirds receive at least four prenatal visits, many of these services are inadequate.
That is why today we not only continue to insist on increasing access, coverage and quality of emergency obstetric care to end preventable maternal mortality. We also emphasize protecting the well-being of pregnant women. This is reflected in the Sustainable Development Goals, the Global Strategy for Women's, Children's and Adolescents' Health, numerous guidelines, the Respectful Maternity Care Charter, and new conceptual frameworks for maternal well-being.
What about newborn health? The challenge of getting through the first month of life
Newborn health has always been conceptually linked to maternal health. Even so, historically, it has historically been relegated to the background. For a long time it was erroneously believed that reducing the 4 million neonatal deaths (in the first month of life) that occurred annually required a financial investment and technical capacity that was unattainable for low-income countries. However, this perception began to change in 1999, when a study showed that simple interventions developed by community health workers in India could reduce neonatal mortality by 50%. Since then, efforts such as the Saving Newborn Lives initiative by Save the Children and the Bill & Melinda Gates Foundation, inclusion in the MDGs and a series of articles in the Lancet in 2005 helped neonatal mortality begin to receive the attention it deserved.
By the time this turning point occurred, the delay was already evident in the neonatal mortality figures. These, over the years, were declining at a slower rate than those for maternal or under-five mortality. In fact, in 2013, 44% of under-five deaths were neonatal deaths.
UNICEF and WHO responded to this in 2014 with the Every Newborn action plan. The goal? To reduce neonatal mortality to below 10 per 1000 live births by 2035, in all countries. By 2024, in addition, neonatal coverage in emergency care standards has been expanded. All this has had a positive effect, contributing to a sustained reduction that continues to this day, although in sub-Saharan Africa or lower income countries it still stands at 26 per 1000 live births.
🧠 Let's pause and reflect
Given the evidence that home-based neonatal care and sepsis management by community workers can reduce neonatal mortality by 62%, under what conditions does it make sense to move certain neonatal care from the formal health system to the community, and what are the risks and opportunities of such a move in humanitarian settings?
- 1Think and write your answer.
- 2Click on «Copy and open».
- 3Paste to receive feedback.
📚 This is the NotebookLM for this topic. It uses only carefully selected references. | What is NotebookLM?
Maternal and neonatal mortality in humanitarian crises and emergency obstetric care (EmONC)
In contexts of humanitarian crisis, two-thirds of maternal deaths and around half of neonatal deaths are concentrated. It is the result of violence, food insecurity, epidemics and the collapse of essential health services.
For this reason, the MISP (Minimum Initial Service Package for Sexual and Reproductive Health in Crisis Situations) includes, along with care for gender-based violence, STIs, abortion and contraception, emergency obstetric and newborn care. This combination of actions is designed to protect the right to life, particularly among women and girls, before being able to expand to more complete and comprehensive care once the initial emergency phase is over.
Emergency obstetric and newborn care (EmONC) is essential for safe delivery.
The most vulnerable times for women and newborns are childbirth and the first day of life. This brief period accounts for 46% of all maternal deaths and 40% of all neonatal deaths (in the first month of life). Therefore, access to quality health care is key to guarantee safe delivery, management of any obstetric complications that may arise, and care for small and vulnerable newborns.
But how to determine which essential services are the highest priority? To define them and facilitate their monitoring in low- and middle-income countries, the emergency obstetric care framework was published in 1997. This framework, updated in 2009 and revised again in 2024, proposes a series of essential functions that should be covered at three levels of care.
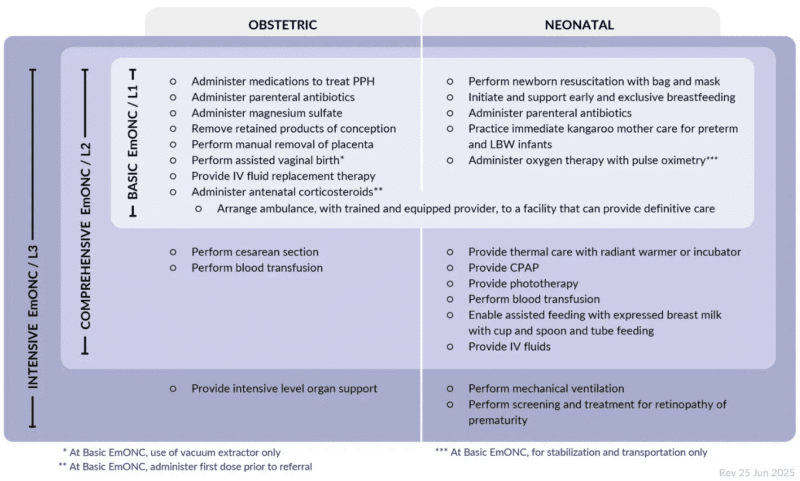
Levels of emergency obstetric and neonatal care: basic, comprehensive and intensive.
The most basic level (BEmONC) should be available in at least 4 centers per 500,000 people and cover at least the following functions:
- Administration of drugs to treat postpartum hemorrhage.
- Administration of parenteral antibiotics to the mother.
- Administration of magnesium sulfate (to prevent seizures in preeclampsia and eclampsia).
- Removal of retained products of conception.
- Manual removal of the placenta.
- Assisted vaginal delivery (only with vacuum extractor).
- Provision of intravenous fluid replacement therapy (to the mother).
- Administration of the first dose of antenatal corticosteroids prior to referral (to improve fetal lung maturation in preterm labor), while coordinating emergency transport with a trained and equipped provider to a facility that can provide definitive care.
- Neonatal resuscitation with bag and mask.
- Initiation and support of early and exclusive breastfeeding.
- Administration of parenteral antibiotics to the newborn. This, together with good hand hygiene practice, is essential for infection prevention.
- Immediate practice of kangaroo mother care for preterm and low birth weight infants.
- Administration of oxygen therapy with pulse oximetry to the neonate, only for stabilization and transport.
Along with these four centers, and for that population figure, there should be at least one hospital offering the complete level (CEmONC):
- Cesarean section.
- Blood transfusion to the mother and newborn.
- Thermal care with radiant warmer or incubator.
- Administration of oxygen therapy with pulse oximetry.
- Continuous positive airway pressure (CPAP).
- Phototherapy.
- Assistance in feeding the newborn with expressed breast milk, using cup and spoon, and tube feeding.
- Intravenous fluids to the neonate.
The 2024 update also proposes a third level to provide intensive care for the mother, mechanical ventilation for the newborn and screening and treatment of retinopathy of prematurity.
Other additional priority needs of the mother and newborn must be met
In addition to emergency obstetric and neonatal care, there are other actions with a high impact on reducing maternal mortality. These include care for abortions in progress and the establishment of a referral system available 24 hours a day, including means of communication and transportation. The latter ensures that women in the community can reach obstetric care in health centers and hospitals on time. In addition, in more complex contexts with limited access to health services, it may be necessary to distribute clean delivery kits to all pregnant women. Both volunteers and women's groups can be responsible for making these kits, or for identifying visibly pregnant women in need of them.
All of these actions and priorities must always be framed by reproductive health, addressed both by supporting or strengthening health systems and by community engagement and mobilization. All components of the MISP are essential to address interconnected life-saving needs, such as contraception, care for survivors of sexual and gender-based violence, childbirth care, or abortion care.
Likewise, these problems cannot be addressed with a vertical vision. All these actions should ideally connect with prenatal care, postnatal follow-up and the rest of the preventive and curative services of primary health care, whenever possible, for greater protection and wellbeing of the mother and newborn. From this primary health care strategy, it is also possible to weave networks of community health workers, traditional birth attendants and women's groups that identify danger signs, promote childbirth in health centers, carry out home visits or protect exclusive breastfeeding.
🧠 Let's pause and reflect
With the new WHO definition (2025) extending the maternal wellness period to one year after pregnancy, how should humanitarian programs adapt to go beyond preventing death and ensure that women thrive physically and mentally?
- 1Think and write your answer.
- 2Click on «Copy and open».
- 3Paste to receive feedback.
📚 This is the NotebookLM for this topic. It uses only carefully selected references. | What is NotebookLM?
Protecting maternal well-being: beyond survival
Fortunately, thanks to many efforts at all levels, maternal mortality figures are decreasing. Therefore, in places where survival is already an achieved goal, a broader approach must be adopted that seeks complete well-being during this period.
The pursuit of maternal wellness requires respectful care that ensures a positive experience during pregnancy, childbirth and postpartum. To this end, quality prenatal care plays a crucial role. On the one hand, it constitutes an important avenue for identifying obstetric complications. On the other hand, prenatal care is also a wonderful gateway to preparing for childbirth, empowering expectant parents for nurturing care, psychosocial support, and addressing maternal health problems such as depression and anxiety.
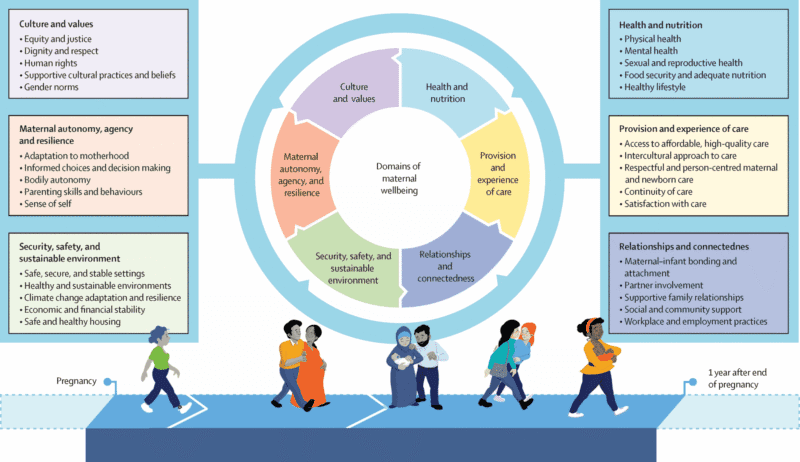
Protecting health and nutrition determinants and ensuring access to reproductive health services are fundamental for maternal well-being. However, coverage, accessibility, and quality of care (delivered respectfully and person-centered) are equally essential. Moreover, this well-being does not depend solely on health services. It also relies on factors such as safety, economic and financial stability, and the sustainability of the living environment, increasingly affected by climate change. Relationships with the baby, family, and community, women’s autonomy, and, of course, gender equity and social justice are also key.
NotebookLM
You can review my bibliographic references on maternal and newborn health with this NotebookLM, an artificial intelligence-based research assistant. Want to know more?
How to cite this page
Abarca, B. (June 29, 2026). Maternal and newborn health in humanitarian settings: history, mortality, EmONC and maternal well-being. Salud Everywhere. https://saludeverywhere.com/en/health-in-humanitarian-crises/maternal-and-newborn-health/
External links
- WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division, 2025. Trends in maternal mortality 2000 to 2023: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division.
- Le Lez, 2025. Maternal wellbeing: a WHO definition and conceptual framework.
- Columbia Mailman School of Public Health and London School of Hygiene and Tropical Medicine, 2024. EmONC Digital Guide.
- IAWG on Reproductive Health in Crises, 2023. Basic Emergency Obstetric and Newborn Care (BEmONC) in Crisis Settings, Select Signal Functions.
- IAWG on Reproductive Health in Crises, 2022. Success Depends on Collaboration: Cross-Sector Technical Brief on Maternal and Newborn Health and Nutrition in Humanitarian Settings.
- WHO, 2022. WHO recommendations on maternal and newborn care for a positive postnatal experience.
- IAWG on Reproductive Health in Crises, 2022. Approaching Implementation of Respectful Maternity Care in Humanitarian Settings.
- WRC, IAWG, 2021. Minimum Initial Service Package MISP For Sexual and Reproductive Health (SRH) in Crisis Situations: a Distance Learning Module. Unit 5: Prevent Excess Maternal and Newborn Mortality and Morbidity.
- Save the Children, UNICEF, UNHCR, and WHO, 2020. Roadmap to Accelerate Progress for Every Newborn in Humanitarian Settings 2020-2024.
- WHO and UNICEF, 2019. Survive and Thrive: Transforming Care for Every Small and Sick Newborn.
- IAWG, 2018. Inter-agency field manual on reproductive health in humanitarian settings.
- Save the Children, UNICEF, and WHO, 2016. Newborn Health in Humanitarian Settings: Field Guide.
- WHO, 2016. WHO recommendations on antenatal care for a positive pregnancy experience.
- Koblinsky, 2016. Quality maternity care for every woman, everywhere: a call to action.
- Otolorin, 2015. Essential basic and emergency obstetric and newborn care: From education and training to service delivery and quality of care.
- WHO, 2014. Every Newborn: an action plan to end preventable deaths.
- Darmstadt, 2014. Who has been caring for the baby?
- AbouZahr, 2003. Safe motherhood: a brief history of the global movement 1947-2002.
- AbouZahr and Wardlaw, 2001. Maternal mortality at the end of a decade: signs of progress?
- Maine and Rosenfield, 1999. The Safe Motherhood Initiative: why has it stalled?
- Bang, 1999. Effect of home-based neonatal care and management of sepsis on neonatal mortality: field trial in rural India.
- Rosenfield and Maine, 1985. Maternal mortality-a neglected tragedy: Where is the M in MCH?