Mental health and psychosocial support (MHPSS) in humanitarian crises
- Page updated onJune 29, 2026
For years, mental health was the great forgotten area of humanitarian response. Today, however, we know that 1 in 5 people affected by conflicts and emergencies suffer from a mental disorder, and that the suffering makes it difficult for them to function, survive and support their families and communities.
Responding to these needs requires a cross-cutting, multisectoral approach to mental health and psychosocial support (MHPSS), covering everything from psychosocial considerations that avoid doing further harm, to strengthening community and social networks, individualized quality care even in the absence of specialists, and specialized clinical care for people with more severe functional impairment.
Table of contents:
What is mental health and psychosocial support?
Epidemiology of mental health in humanitarian and resource-poor settings
For years, mental health took a back seat in the humanitarian response. Today, however, we are aware of its importance. It is estimated that 1 in 5 people (22%) affected by conflict and crisis suffer from some mental disorder. Of these, 13% suffer from mild forms of depression, anxiety or post-traumatic stress disorder (PTSD), while 9% suffer from moderate and severe disorders.
In general populations, mood disorders affect 5.3% of the population. In humanitarian crises, this figure rises to 17.31%. Similarly, the prevalence of anxiety and PTSD rises from 7.61% to 15.41%. These figures, however, should not be analyzed solely from a biomedical approach. These disorders have a great impact on the functional impairment of individuals, who see their ability to perform daily activities or play essential roles for their survival and that of their families and communities reduced.
These problems result from the interaction between individual factors (genetics, age, gender), exposure to traumatic events and the cumulative impact of daily stressors. In humanitarian contexts, extreme poverty, homelessness, displacement, food insecurity, gender violence and lack of access to basic health or education services, among other social determinants of health are aggravated. Some groups, moreover, face even greater risks, such as people with disabilities, unaccompanied children and survivors of torture, as well as refugees and caregivers of children with illnesses or acute malnutrition.
Added to all this is the huge gap between need and response. In low- and middle-income countries, less than 20% of people with mental disorders receive quality care. This disparity, moreover, is exacerbated in complex humanitarian crises.
Mental health and psychosocial support: a link between health and protection
To respond to these needs, in 2007, the Inter-Agency Standing Committee (IASC) Working Group on Mental Health and Psychosocial Support in Emergency Settings published a technical guide. This document would represent a turning point in the approach to mental health in humanitarian crises, not only by bringing to the forefront a historically neglected priority, but also by doing so from a completely new conceptual and operational framework.
The 2007 consensus was a reflection of an idea: social support is essential to protect and support mental health and psychosocial well-being. Thus a new term emerged: Mental Health and Psychosocial Support (MHPSS). Under it, two complementary and closely related approaches were combined:
- The healthcare approach: traditionally focused on the prevention and treatment of mental and neurological disorders.
- The protection, education and social services approach: more related to welfare and alleviation of suffering through the strengthening of family and community networks and the modification of the social environment in which people live.
The new term, however, has not been without confusion and disagreement. Although psychosocial support has traditionally been understood as “non-pharmacological intervention” in the health sector, in this case it refers to a broad spectrum of socio-environmental and relational interventions. What this new common language has generated consensus on, in any case, is the cross-cutting and multisectoral vision of mental health. At the same time, it has been key in helping to make visible operational needs and priorities that were previously invisible.
Approaching mental health from four complementary levels: the MHPSS pyramid
The Mental Health and Psychosocial Support in Emergency Situations guide of 2007 became, over time, the most influential tool on this topic in the humanitarian sector. It proposed four complementary levels of care:
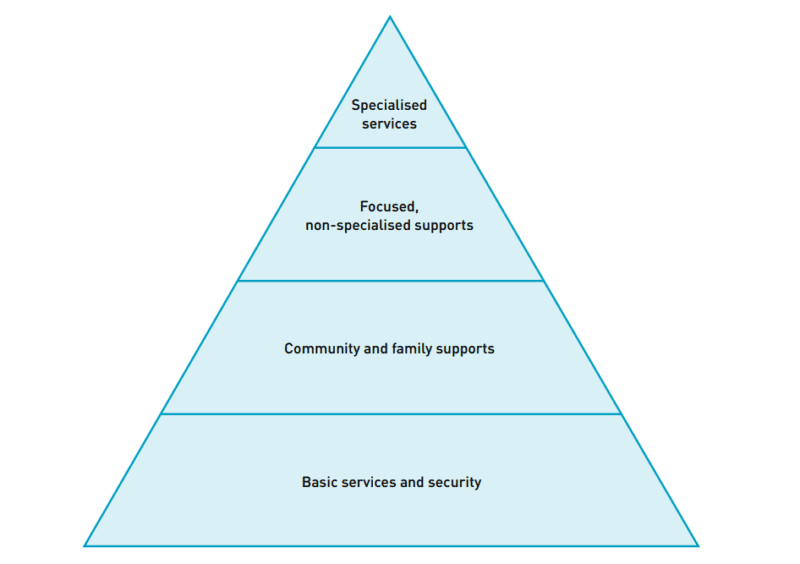
- Level 1: Basic services and security. The base of the pyramid focuses on promoting the well-being of the entire population. To this end, it is proposed that, from all sectors of humanitarian action, key considerations should be adopted to ensure that their assistance is dignified, safe and culturally appropriate.
- Level 2: Family and community support. The second level focuses on the activation and protection of social support networks, self-help and community cohesion. This level recognizes the importance for the mental health of the population of the existence of child-friendly spaces or efforts to reunite families separated by the crisis, among other examples.
- Level 3: Non-specialized focused support. This level prioritizes attention to a smaller group of people, who are those requiring more direct interventions. These interventions include, for example, psychological first aid, some group activities led by well-trained and supervised staff, or basic mental health care by primary care health personnel.
- Level 4: Specialized services. This last level requires specialists such as psychiatrists or psychologists with sufficient training and experience to be able to care for people with severe functional impairment and intolerable suffering.
Rather than confining different actors to rigid roles, this classification aims to generate synergy across organizations. It also provides a framework to facilitate the flow of individuals between levels of care that must be addressed simultaneously through an effective referral and counter-referral system.
How can we measure mental health status?
The way of measuring, monitoring and evaluating mental health has also evolved, to go much further than counting symptoms of different psychiatric disorders. In this regard, current frameworks focus on six indicators:
- The functioning or ability to perform essential daily activities.
- The subjective perception of well-being, security, calm and hope.
- The presence of severe disorders or symptoms that produce disabling distress.
- The coping, problem-solving and stress management skills.
- The social behavior, such as aggressiveness, violence or attitude of helping other people.
- The social connectivity, through support networks and family and community circles.
In humanitarian practice, however, there is some tension around needs assessments. Despite the traditional impulse to count people with clinical disorders, it is now realized that diagnostic tools are not always locally adaptable and that we already have sufficient information to justify immediate action on mental health and psychosocial support in any humanitarian crisis.
Moreover, it is stressed that, in many cases, it may be more important to understand how the crisis affects people's functionality and what local capacity exists. For the latter, it is essential to map well the resources available at each level, as well as the coping mechanisms of the population or the community-based structures that serve as mutual aid.
How has MHPSS in emergencies continued to evolve?
Evolution of MHPSS in the 21st century: from vertical to systemic
The new approach to mental health and psychosocial support proposed in 2007 was a turning point, which was followed by further changes and advances. These included the Mental Health Gap Action Program (mhGAP), published by the WHO in 2008. Under this action plan, and closely related to the interrelationship between the levels of the IASC pyramid, it was proposed to advance the integration of mental health into primary health care and universal health coverage. This required strengthening the capacities of non-specialized health personnel as a prerequisite for delegating key functions to them. There were also initiatives to drive this change in the reconstruction phase of health systems after acute emergencies, as was the case in Sri Lanka after the 2004 tsunami.
Over the years, MHPSS has been mainstreamed into humanitarian action. An example of this was its inclusion in the 2018 update of the Sphere Handbook, or the psychosocial gaze that permeated the response to the COVID-19 pandemic in many contexts.
Since then, major historical gaps in the operationalization of MHPSS were also filled, with the publication of monitoring frameworks and a Minimum Service Package in 2022. In this same period, WHO urged Member States to invest in MHPSS, in its inclusion in emergency preparedness and response plans, and in decentralization to community levels.
Towards mental health empowerment in primary care and community health workers
The 2020s have seen a revitalized interest in community and community health workers programs. These community volunteers, but recognized by the humanitarian system and national and local public institutions, have demonstrated enormous potential to boost access to health and wellness. This trend has also been mirrored in mental health and psychosocial support, as had already been driving since 2008 with the mhGAP.
Gradually, more and more evidence has been accumulating that non-specialized and volunteer staff can deliver psychological interventions with results comparable to those of specialists and much greater potential for scalability. This model of intervention may not only be more cost-effective, but also contributes to reducing the stigma associated with mental health and addressing functional impairment from within homes and communities.
These models do not displace specialized mental health personnel. Their role does not disappear but is transformed. Thus, assuming that the shortage of psychiatrists and psychologists is a reality, they can multiply their impact by training, supervising, accompanying and caring for front-line teams, which need resources and technical support.
🧠 Let's pause and reflect
How do we prevent the integration of mental health and psychosocial support in primary care from becoming an unbearable overload for frontline health workers already managing malnutrition crises or infectious outbreaks?
- 1Think and write your answer.
- 2Click on «Copy and open».
- 3Paste to receive feedback.
📚 This is the NotebookLM for this topic. It uses only carefully selected references. | What is NotebookLM?
Mental health is now a cross-cutting issue in humanitarian action
Mental health and psychosocial considerations in all sectors
The way in which humanitarian aid is implemented matters. Therefore, all sectors must take into account certain considerations. These include protecting people's dignity and privacy, fostering their autonomy and sense of control over their own lives, mitigating social stressors such as lack of adequate water or shelter, and identifying people with acute distress for referral to focused support services and specialized care.
It is worth highlighting some specific examples in different sectors:
- Water, sanitation and hygiene. The lack of privacy and safety of latrines in settlements and refugee camps may partly determine the risk of sexual violence.
- Nutrition. Caregiver distress can have serious repercussions on caregiving and child feeding practices. Facing difficult situations of displacement and violence can hinder the practice of breastfeeding or providing loving care and stimulation.
- Coordination and management of camps for displaced persons. Community participation (women, men, girls and boys) in camp design and settlement management has been shown to promote social cohesion and reduce feelings of helplessness.
- Education. Schools should be a safe space for children, who can find in them a routine, leisure and sense of normality with important therapeutic effects and for their well-being and development.
Beyond the guidelines and recommendations, however, important challenges remain to “de-medicalize” the suffering of people in humanitarian crises. At times, humanitarian funding models continue to incentivize the prioritization of immediate results or the possibility of counting more beneficiaries, regardless of the complexity and importance of how this is done.
Minimum package of mental health and psychosocial support services
In 2022, the IASC proposed a minimum package of top priority mental health and psychosocial support services in humanitarian crises. The objectives of these multisectoral actions are to stabilize the population, help them regain their capacity for basic functioning, reduce acute stress, and prevent the onset or worsening of serious mental disorders. To this end, the aim is to provide an environment of safety and human support, in a well-coordinated manner across sectors.
Orientation of humanitarian actors and community members on MHPSS
This block of actions is the heart of the multisectoral mental health response, and addresses both the sensitization of actors to take into account basic psychosocial considerations in their interventions, as well as support to personnel on the front line of assistance to people affected by the crisis.
From the onset of the crisis, it is important that decision makers, humanitarian professionals and community leaders understand the importance of mental health and psychosocial support. Mental health needs to be placed high on the agendas of inter-sectoral coordination and government authorities.
This block also includes the preparation of personnel and front-line community agents so that they have basic skills in psychosocial support for people with acute distress. They should be trained in psychological first aid. It is important to clarify that this is not therapy or a single-session psychological debriefing (which could even be harmful). Psychological first aid consists of listening without pressuring the person, assessing basic needs of any kind, protecting from further harm, and connecting to available services that are a priority, such as food, protection, or shelter.
Community strengthening and group support
This block stems from the recognition that the people of the community themselves have the deepest knowledge of the local culture and resources. It includes actions such as the following:
- Dissemination of key messages. This helps to normalize reactions to acute stress, encourage positive coping mechanisms and promote resilience. This involves giving simple messages adapted to the local culture, which also include information about people's rights and available services.
- Support for community activities. There may be support networks and initiatives among people with shared interests that we should try to protect and strengthen. This helps people regain their functional capacity, as well as fostering a sense of collective identity and mutual aid.
- Promote early child development and loving and sensitive care. This can be done by creating baby-friendly spaces, where caregivers can be supported in positive parenting, infant care and feeding.
- Structured group activities with children and adolescents. In safe spaces for children, games and activities can be conducted that offer protection and psychosocial well-being, as well as an opportunity to identify those with specific protection needs.
- Promoting the well-being of caregivers and their ability to support children. Caring for caregivers is a priority that must be addressed at the same time as everything else.
- Supporting educational staff. They are often under great stress. Therefore, they must be protected and trained in social and emotional learning.
- Offer MHPSS in safe spaces for girls and women. These actions also reduce the risk and consequences of gender-based violence.
Focused, clinical support for people affected by distress or mental health conditions
This block focuses on levels 3 and 4 of the MHPSS intervention pyramid. Therefore, it targets the subpopulation suffering from significant functional impairment or mental, neurological and substance use disorders.
This includes the integration of mental health into primary health care. To this end, there are protocols and training frameworks such as the mhGAP, so that non-specialized health personnel can treat conditions such as psychosis, depression, anxiety or epilepsy (which also requires access to essential psychotropic drugs). Also proposed at this level is the integration of MHPSS in the services of care for survivors of sexual and gender-based violence, in the individualized management of protection cases and in the care of institutionalized persons.
In humanitarian contexts where specialized personnel are scarce or non-existent, non-specialized but well-trained and supervised personnel can also offer scalable psychological interventions. These are interventions laid out in manuals with precise step-by-step instructions and a transdiagnostic approach, addressing a variety of problems such as stress, fear and sadness at once. These include Problem Management Plus (focused on adults with depression or anxiety), Thinking Healthy (aimed at mothers with perinatal depression), Early Adolescent Skills for Emotions (or EASE), Self-Help Plus (a group intervention for stress management), and even other self-help interventions guided by digital tools and artificial intelligence.
🧠 Let's pause and reflect
Under what ethical and technical criteria should a coordinator decide which activity of the MHPSS minimum service package to implement first when resources do not allow to cover them all simultaneously?
- 1Think and write your answer.
- 2Click on «Copy and open».
- 3Paste to receive feedback.
📚 This is the NotebookLM for this topic. It uses only carefully selected references. | What is NotebookLM?
The sustainable transformation of mental health systems
Consistent with the development-humanitarian-peace nexus approach, in emergencies and crises we can not only respond to the most immediate needs, but also catalyze long-term development.
This idea of “building back better” the mental health system, however, must be thought out and planned from day one, as in other health actions. Thus, it is possible to avoid creating systems parallel to the existing health system and national structures, and to promote the integration of mental health into primary care and community health, with good specialized supervision. Experience seems to show that the chances of success increase with horizontal approaches that do not focus on a specific pathology and with investment in people and communities. Thus, short-term efforts, over time, can result in real systemic change, with sustainable future positive effects on the mental health and well-being of the population.
NotebookLM
You can review my literature references on mental health and psychosocial support in humanitarian crises with this NotebookLM, an artificial intelligence-based research assistant. Do you want to know more?
How to cite this page
Abarca, B. (June 29, 2026). Mental health & psychosocial support (MHPSS) in humanitarian crises. Salud Everywhere. https://saludeverywhere.com/en/humanitarian-aid-and-international-development/mental-health-and-psychosocial-support-in-humanitarian-crises/
External links
- ELRHA, IFRC, 2025. Evidence from the frontline: Mental health in crisis affected contexts (podcasts).
- OpenWHO, 2024. Introducing mental health and psychosocial support in emergencies (videos).
- WHO, 2024. Psychological interventions implementation manual: integrating evidence-based psychological interventions into existing services.
- WHO, 2023. Mental Health Gap Action Programme (mhGAP) guideline for mental, neurological and substance use disorders.
- People’s Health Movement, 2023. Transforming mental healthcare globally.
- IASC, 2022. The Mental Health and Psychosocial Support Minimum Service Package.
- IASC, 2022. IASC Handbook, Mental Health and Psychosocial Support Coordination.
- IASC, 2022. Guidance Note: Addressing Suicide in Humanitarian Settings.
- IASC, 2021. The Common Monitoring and Evaluation Framework for Mental Health and Psychosocial Support in Emergency Settings: with means of verification (Version 2.0).
- WHO, 2021. Comprehensive Mental Health Action Plan 2013-2030.
- Miller, 2021. A call for greater conceptual clarity in the field of mental health and psychosocial support in humanitarian settings.
- Ogbe, 2019. A systematic review of intimate partner violence interventions focused on improving social support and/ mental health outcomes of survivors.
- Aldamman, 2019. Caring for the mental health of humanitarian volunteers in traumatic contexts: the importance of organisational support.
- Tol, 2015. Mental health and psychosocial support in humanitarian settings: a public mental health perspective.
- Strohmeier, 2015. Trauma-related mental health problems among national humanitarian staff: a systematic review of the literature.
- IASC, 2014. Review of the Implementation of the IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings.
- IASC, 2012. IASC Reference Group Mental Health and Psychosocial Support Assessment Guide.
- Tol, 2011. Mental health and psychosocial support in humanitarian settings: linking practice and research.
- IASC, 2010. Mental Health and Psychosocial Support in Humanitarian Emergencies: What Should Humanitarian Health Actors Know?
- IASC, 2007. IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings.